Grading of the tumors of the central nervous system
The concept of grading of the tumors of the central nervous system, agreeing for such the regulation of the "progressiveness" of these neoplasias (from benign and localized tumors to malignant and infiltrating tumors), dates back to 1926 and was introduced by P. Bailey and H. Cushing,[1]
in the elaboration of what turned out the first systematic classification of gliomas.[2]
In the following, the grading systems present in the current literature are introduced. Then, through a table, the more relevant are compared.
| Grading of the tumors of the CNS | |
|---|---|
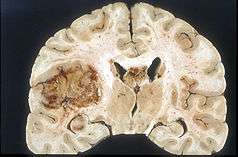
 Glioblastoma arising in an astrocytoma. This spinal cord exhibits both a lightly staining microcystic astrocytoma as well as a darkly staining glioblastoma. | |
| Medicine WikiProject/Neurology task force | |
ICD-O scale
The first edition of the International Classification of Diseases (ICD) dates back to 1893. The current review (ICD-10) dates back to 1994, came into use in the U.S. in 2015, and is revised yearly, being very comprehensive.
In 1976 the World Health Organization (WHO) publishes the first edition of the International Classification of Diseases for Oncology (ICD-O), now at the third edition (ICD-O-3, 2000).
In this last edition, the Arabic numeral after the character "/" indicates the "behavior" of the neoplasia, with the following meaning:[3]
- /0 benign neoplasia
- /1 uncertain neoplasia (benign or malignant)
- /2 neoplasia in situ
- /3 primary infiltrative malignant neoplasia
- /6 secondary malignant neoplasia
- /9 malignant neoplasia, uncertain if primitive or secondary
For the concepts of benign and malignant neoplasia see Tumor and Cancer.
For primary and secondary neoplasias see Metastasis.
A brain tumor composed of benign cells, but located in a vital area (as the brain is), can be considered to be life-threatening — although the tumor and its cells would not be classified as malignant.
Kernohan grading
The Kernohan grading system[4][5] defines progressive malignancy of astrocytomas as follows:
- Grade 1 tumors are benign astrocytomas.
- Grade 2 tumors are low-grade astrocytomas.
- Grade 3 tumors are anaplastic astrocytomas.
- Grade 4 tumors are glioblastomas.
St Anne-Mayo grading
The St Anne-Mayo grading system[4][6][7] also is used to grade astrocytomas; however, this system uses four morphologic criteria to assign a grade:
a) nuclear atypia,
b) mitosis,
c) endothelial proliferation-'piled-up' endothelial cells. NOT hypervascularity
d) necrosis.
The St. Anne-Mayo grade has four categories of tumors:
- Grade 1 tumors do not meet any of the criteria.
- Grade 2 tumors meet one criterion, usually nuclear atypia.
- Grade 3 tumors meet two criteria, usually nuclear atypia and mitosis.
- Grade 4 tumors meet three or four of the criteria.
WHO grading
The World Health Organization (WHO) grading system[4][8][9][10] is contained in the volume Histological Typing of Tumours of the Central Nervous System, whose first edition dates back to 1979, the second to 1993 and last one to 2007. The WHO grade has four categories of tumors:
- Grade I tumors are slow-growing, nonmalignant, and associated with long-term survival.
- Grade II tumors are relatively slow-growing but sometimes recur as higher grade tumors. They can be nonmalignant or malignant.
- Grade III tumors are malignant and often recur as higher grade tumors.
- Grade IV tumors reproduce rapidly and are very aggressive malignant tumors.
From the histological point of view the WHO system is based on the same criteria as the St Anne-Mayo system.[11][12]
Comparison of the grading systems
In the following table the various grading systems are compared (the IDC-O scale is not comprised because it is not considered a real grading system):[13][14][15]
| Nome WHO | WHO grade | Kernohan grade | St Anne/Mayo grade | St Anne/Mayo criteria |
|---|---|---|---|---|
| Pilocytic astrocytoma | I | - | 1 | 0 criterion |
| Diffuse astrocytoma | II | 1/2 | 2 | 1 criterion (a) |
| Anaplastic astrocytoma | III | 3 | 3 | 2 criteria (a+b) |
| Glioblastoma | IV | 4 | 4 | 3-4 criteria (a+b[+/-c]+d) |
Notes
References
-
Bailey P, Cushing H (1926).
A classification of the tumors of the glioma group on a histogenic basis with a correlated study of prognosis.
J B Lippincott Co. Philadelphia. -
Tonn J-C, Westphal M, Rutka JT, Grossman SA (2006).
Neuro-Oncology of CNS Tumors
Springer Science & Business, ISBN 3-540-25833-7. - Vicari P (2007).
Principi di codifica delle neoplasie.
Reggio Emilia dicembre 2007. Accessed on 2009-08-12. -
Centers for Disease Control and Prevention (2004).
Data collection of primary central nervous system tumors. National Program of Cancer Registries Training Materials.
Atlanta, Georgia: Department of Health and Human Services, Centers for Disease Control and Prevention. -
Kernohan JW, Mabon RF, Svien HJ, Adson AW (1949).
A Semplified classification of gliomas.
Proc. Staff: Meet. Mayo Clin. 24: 71-75. -
Daumas-Duport C, Scheithauer B, O'Fallon J, Kelly P (1988).
Grading of astrocytomas. A simple and reproducible method.
Cancer 62: 2152-2165. -
Kim TS, Halliday AL, Hedley W, Convery K (1991).
Correlates of survival and the Daumas-Duport grading system for astrocytomas.
J Neurosurg 74: 27-37. -
Kleihues P, Burger PC, Scheithauer BW (1993).
Histological Typing of Tumours of Central Nervous System. World Health Organization International Histological Classification of Tumours.
2nd ed. Springer Verlag: Berlin Heidelberg. -
Kleihues P, Kiessling M, Scheithauer BW (1987).
The new WHO classification of brain tumours.
Brain Pathol. 3: 255-268. - Acta Neuropathol. 2007 Aug;114(2):97-109. Epub 2007 Jul 6. The 2007 WHO classification of tumours of the central nervous system. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P. Source Department of Pathology, Massachusetts General Hospital and Harvard Medical School, Boston, MA 02114, USA.
-
Grier JT, Batchelor T (2006).
Low-Grade Gliomas in Adults
Oncologist. 2006 Jun;11(6):681-93. -
Buckner JC, Brown PD, O'Neill BP, Meyer FB, Wetmore CJ, Uhm JH (2007).
Central nervous system tumors.
Mayo Clin Proc. 2007 Oct;82(10):1271-86. -
Tatter SB (2005).
The new WHO Classification of Tumors affecting the Central Nervous System.
Accessed on 2009-08-12. -
Gudinavičienė I (2004).
Impact of morphology and biology on the prognosis of patiens with gliomas.
Medicina Vol. 40, No. 2. -
Kleihues P, Cavenee WK, eds. (2000).
Pathology and genetics of tumours of the nervous system. World Health Organization classification of tumours.
Lyon, France: IARC Press ISBN 92-832-2409-4.
Bibliography
- Kleihues P, Cavenee WK, eds. (2000). Pathology and genetics of tumours of the nervous system.
World Health Organization classification of tumours. Lyon, France: IARC Press ISBN 92-832-2409-4. - Louis DN, Ohgaki H, Wiestler OD, Cavenee WK (eds) (2007). World Health Organization Classification of Tumours of the Central Nervous System. IARC, Lyon ISBN 92-832-2430-2.
External links
- AFIP Course Syllabus - Astrocytoma WHO Grading Lecture Handout