Thought disorder
Thought disorder (TD) refers to disorganized thinking as evidenced by disorganized speech.[1] Specific thought disorders include derailment, poverty of speech, tangentiality, illogicality, perseveration, and thought blocking.[1]
| Thought disorder | |
|---|---|
| Other names | Formal thought disorder (FTD) |
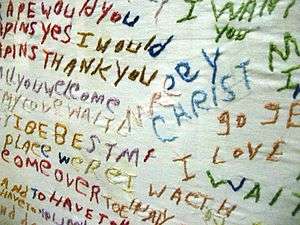 | |
| An embroidered cloth produced by a schizophrenia patient, showing the nonsensical associations between words and ideas characteristic of thought disorder | |
| Specialty | Psychiatry |
Psychiatrists consider formal thought disorder as being one of two types of disordered thinking, with the other type being delusions. The latter involves "content" while the former involves "form". Although the term "thought disorder" can refer to either type, in common parlance it refers most often to a disorder of thought "form" also known as formal thought disorder.
Eugen Bleuler, who named schizophrenia, held that thought disorder was its defining characteristic.[2] However, formal thought disorder is not unique to schizophrenia or psychosis. It is often a symptom of mania, and less often it can be present in other mental disorders such as depression.[1] Clanging or echolalia may be present in Tourette syndrome.[3] Patients with a clouded consciousness, like that found in delirium, also have a formal thought disorder.[4]
However, there is a clinical difference between these two groups. Those with schizophrenia or psychosis are less likely to demonstrate awareness or concern about the disordered thinking.[5] Clayton and Winokur have suggested that this results from a fundamental inability to use the same type of Aristotelian logic as others.[6] On the other hand, patients with a clouded consciousness, referred to as "organic" patients, usually do demonstrate awareness and concern, and complain about being "confused" or "unable to think straight"; Clayton and Winokur suggest that this is because their thought disorder results, instead, from various cognitive deficits.[4]
Signs and symptoms
In considering whether an individual has thought disorder, patterns of their speech are closely observed. Although it is normal to exhibit some of the following during times of extreme stress (e.g. a cataclysmic event or the middle of a war) it is the degree, frequency, and the resulting functional impairment that leads to the conclusion that the person being observed has a thought disorder.[7][8]
- Alogia (also poverty of speech) – A poverty of speech, either in amount or content; it can occur as a negative symptom of schizophrenia.[1]
- Blocking – An abrupt stop in the middle of a train of thought; the individual may or may not be able to continue the idea.[9] This is a type of formal thought disorder that can be seen in schizophrenia.[1]
- Circumstantiality (also circumstantial thinking, or circumstantial speech) – An inability to answer a question without giving excessive, unnecessary detail.[9] This differs from tangential thinking, in that the person does eventually return to the original point.
- Clanging or Clang association – a severe form of flight of ideas whereby ideas are related only by similar or rhyming sounds rather than actual meaning.[9] This may be heard as excessive rhyming and/or alliteration. e.g. "Many moldy mushrooms merge out of the mildewy mud on Mondays." "I heard the bell. Well, hell, then I fell." It is most commonly seen in bipolar affective disorder (manic phase), although it is often observed in patients with primary psychoses, namely schizophrenia and schizoaffective disorder.
- Derailment (also loose association and knight's move thinking) – Thought and/or speech move, either spontaneously or in response to an internal stimulus (distinguishing derailment from "distractible speech," infra), from the topic's track onto another which is obliquely related or unrelated.[9] e.g. "The next day when I'd be going out you know, I took control, like uh, I put bleach on my hair in California."
- Distractible speech – During mid speech, the subject is changed in response to an external stimulus. e.g. "Then I left San Francisco and moved to... where did you get that tie?"
- Echolalia – Echoing of another's speech[9] that may only be committed once, or may be continuous in repetition. This may involve repeating only the last few words or last word of the examiner's sentences. This can be a symptom of Tourette's Syndrome. e.g. "What would you like for dinner?", "That's a good question. That's a good question. That's a good question. That's a good question."
- Evasive interaction – Attempts to express ideas and/or feelings about another individual come out as evasive or in a diluted form, e.g.: "I... er ah... you are uh... I think you have... uh-- acceptable erm... uh... hair."
- "Flight of ideas" – a form of formal thought disorder marked by abrupt leaps from one topic to another, albeit with discernable links between successive ideas, perhaps governed by similarities between subjects or, in somewhat higher grades, by rhyming, puns, and word plays (clang associations), or innocuous environmental stimuli – e.g., the sound of birds chirping. It is most characteristic of the manic phase of bipolar illness.
- Illogicality – Conclusions are reached that do not follow logically (non-sequiturs or faulty inferences). e.g. "Do you think this will fit in the box?" draws a reply like "Well duh; it's brown, isn't it?"
- Incoherence (word salad) – Speech that is unintelligible because, though the individual words are real words, the manner in which they are strung together results in incoherent gibberish,[9] e.g. the question "Why do people comb their hair?" elicits a response like "Because it makes a twirl in life, my box is broken help me blue elephant. Isn't lettuce brave? I like electrons, hello please!"
- Loss of goal – Failure to follow a train of thought to a natural conclusion. e.g. "Why does my computer keep crashing?", "Well, you live in a stucco house, so the pair of scissors needs to be in another drawer."
- Neologisms – New word formations.[9] These may also involve elisions of two words that are similar in meaning or in sound. e.g. "I got so angry I picked up a dish and threw it at the geshinker."
- Perseveration – Persistent repetition of words or ideas even when another person attempts to change the topic.[9] e.g. "It's great to be here in Nevada, Nevada, Nevada, Nevada, Nevada." This may also involve repeatedly giving the same answer to different questions. e.g. "Is your name Mary?" "Yes." "Are you in the hospital?" "Yes." "Are you a table?" "Yes." Perseveration can include palilalia and logoclonia, and can be an indication of organic brain disease such as Parkinson's.
- Phonemic paraphasia – Mispronunciation; syllables out of sequence. e.g. "I slipped on the lice and broke my arm."
- Pressure of speech – Unrelenting, rapid speech without pauses.[9] It may be difficult to interrupt the speaker, and the speaker may continue speaking even when a direct question is asked.
- Self mentions – Patient repeatedly and inappropriately refers back to self. e.g. "What's the time?", "It's 7 o'clock. That's my problem."
- Semantic paraphasia – Substitution of inappropriate word. e.g. "I slipped on the coat, on the ice I mean, and broke my book."
- Stilted speech – Speech characterized by the use of words or phrases that are flowery, excessive, and pompous.[9] e.g. "The attorney comported himself indecorously."
- Tangentiality – Wandering from the topic and never returning to it or providing the information requested.[9] e.g. in answer to the question "Where are you from?", a response "My dog is from England. They have good fish and chips there. Fish breathe through gills."
- Word approximations – Old words used in a new and unconventional way. e.g. "His boss was a seeover."
Thought form, content and process
Disorders of thought form
The most common thought form disorders are: circumstantiality, derailment, flight of ideas, illogicality, incoherence, loose associations, perseveration, tangentiality.[10]
Disorders of thought content
The most common disorders of thought content are delusions of various types (e.g. persecutory, grandiose, referential).[11]
Derealization and depersonalization are another type of abnormal thought content that refer to dissociative experiences.[10]
Intrusive thoughts also are examples of altered thought content. The patient experience involuntary obsessional thoughts, images, or unpleasant ideas that are egodystonic.[10]
Diagnosis
The concept of thought disorder has been criticized as being based on circular or incoherent definitions.[12] For example, thought disorder is inferred from disordered speech, based on the assumption that disordered speech arises because of disordered thought. Incoherence, or word salad, refers to speech that is unconnected and conveys no meaning to the listener.[9]
Furthermore, although thought disorder is typically associated with psychosis, similar phenomena can appear in different disorders, potentially leading to misdiagnosis—for example, in the case of incomplete yet potentially fruitful thought processes.
It has been suggested that individuals with autism spectrum disorders (ASD) display language disturbances like those found in schizophrenia; a 2008 study found that children and adolescents with ASD showed significantly more illogical thinking and loose associations than control subjects. The illogical thinking was related to cognitive functioning and executive control; the loose associations were related to communication symptoms and to parent reports of stress and anxiety.[13]
See also
- Agnosia
- Aphasia
- Auditory processing disorder
- Circumstantial speech
- Emil Kraepelin's dream speech
- Schizophasia
- Speech and language pathology
References
- Yudofsky, Stuart C.; Hales, Robert E. (2002). The American Psychiatric Publishing Textbook of Clinical Psychiatry. Washington, DC: American Psychiatric Association. ISBN 1-58562-032-7. OCLC 49576699.
- Colman, A. M. (2001) Oxford Dictionary of Psychology, Oxford University Press. ISBN 0-19-860761-X
- Barrera A, McKenna PJ, Berrios GE (2009). "Formal thought disorder, neuropsychology and insight in schizophrenia". Psychopathology. 42 (4): 264–9. doi:10.1159/000224150. PMID 19521143.
- John Noble; Harry L. Greene (15 January 1996). Textbook of primary care medicine. Mosby. p. 1325. ISBN 978-0-8016-7841-7.
- Jefferson, James W.; Moore, David Scott (2004). Handbook of medical psychiatry. Elsevier Mosby. p. 131. ISBN 0-323-02911-6.
- Clayton, Paula J.; Winokur, George (1994). The Medical basis of psychiatry. Philadelphia: Saunders. pp. 13–14. ISBN 0-7216-6484-9.
- Andreasen NC. Thought, language, and communication disorders. I. A Clinical assessment, definition of terms, and evaluation of their reliability. Archives of General Psychiatry 1979;36(12):1315–21. PMID 496551.
- Sadock, B.J. and Sadock, V.A. Kaplan and Sadock's Synopsis of Psychiatry. 9th ed. 2003: Table 7.1–6 p 239.
- Videbeck, S (2008). Psychiatric-Mental Health Nursing, 4th ed. Philadelphia: Wolters Kluwers Health, Lippincott Williams & Wilkins.
- Chow, Tiffany W.; Cummings, Jeffrey L. "Neuropsychiatry: Clinical Assessment and Approach to Diagnosis". In Sadock, Benjamin J.; Sadock, Virginia A. (eds.). Kaplan & Sadock's Comprehensive Textbook of Psychiatry (7th. ed.). Lippincott Williams & Wilkins Publishers.
- S. Hossein Fatemi; Paula J. Clayton (15 May 2008). The Medical Basis of Psychiatry. Springer Science & Business Media. pp. 435–436. ISBN 978-1-59745-252-6.
- Bentall, R. (2003) Madness explained: Psychosis and Human Nature. London: Penguin Books Ltd. ISBN 0-7139-9249-2
- Solomon M, Ozonoff S, Carter C, Caplan R (2008). "Formal thought disorder and the autism spectrum: relationship with symptoms, executive control, and anxiety". J Autism Dev Disord. 38 (8): 1474–84. doi:10.1007/s10803-007-0526-6. PMC 5519298. PMID 18297385.
Further reading
- Peter J. McKenna; Tomasina M. Oh (2005). Schizophrenic Speech: Making Sense of Bathroots and Ponds that Fall in Doorways. Cambridge University Press. ISBN 978-0-521-81075-3.