Focused assessment with sonography for trauma
Focused assessment with sonography in trauma (commonly abbreviated as FAST) is a rapid bedside ultrasound examination performed by surgeons, emergency physicians, and certain paramedics as a screening test for blood around the heart (pericardial effusion) or abdominal organs (hemoperitoneum) after trauma.[1]
| Focused assessment with sonography in trauma | |
|---|---|
| Medical diagnostics | |
| eMedicine | 104363 |
The four classic areas that are examined for free fluid are the perihepatic space (including Morison's pouch or the hepatorenal recess), perisplenic space, pericardium, and the pelvis. With this technique it is possible to identify the presence of intraperitoneal or pericardial free fluid. In the context of traumatic injury, this fluid will usually be due to bleeding.
Extended FAST
The extended FAST (eFAST) allows for the examination of both lungs by adding bilateral anterior thoracic sonography to the FAST exam. This allows for the detection of a pneumothorax with the absence of normal ‘lung-sliding’ and ‘comet-tail’ artifact (seen on the ultrasound screen). Compared with supine chest radiography, with CT or clinical course as the gold standard, bedside sonography has superior sensitivity (49–99% versus 27–75%), similar specificity (95–100%), and can be performed in under a minute.[2] Several recent prospective studies have validated its use in the setting of trauma resuscitation, and have also shown that ultrasound can provide an accurate estimation of pneumothorax size.[3][4] Although radiography or CT scanning is generally feasible, immediate bedside detection of a pneumothorax confirms what are often ambiguous physical findings in unstable patients, and guides immediate chest decompression. In addition, in the patient undergoing positive-pressure ventilation, the detection of an otherwise ‘occult’ pneumothorax prior to CT scanning may hasten treatment and subsequently prevent development of a tension pneumothorax, a deadly complication if not treated immediately, and deterioration in the radiology suite (in the CT scanner).[5]
Findings
eFAST (extended focused assessment with sonography for trauma) allows an emergency physician or a surgeon the ability to determine whether a patient has pneumothorax, hemothorax, pleural effusion, mass/tumor, or a lodged foreign body. The exam allows for visualization of the echogenic tissue, ribs, and lung tissue. Few radiographic signs are important in any trauma and they include the stratosphere sign, the sliding or seashore sign, and the sinusoid sign.
Stratosphere sign is a clinical medical ultrasound finding usually in an eFAST examination that can prove presence of a pneumothorax. The sign is an imaging finding using a 3.5–7.5 MHz ultrasound probe in the 4th and 5th intercostal spaces in the anterior clavicular line using the M-Mode of the machine. This finding is seen in the M-mode tracing as pleura and lung being indistinguishable as linear hyperechogenic lines and is fairly reliable for diagnosis of a pneumothorax. Even though the stratospheric sign can be an indication of pneumothorax its absence is not at all reliable to rule out pneumothorax as definitive diagnosis usually requires X-ray or CT of thorax.[6][7][8]
Seashore sign is another eFAST finding usually in the lungs in the M-mode that depicts the glandular echogenicity of the lung abutted by the linear appearance of the visceral pleura. This sign is a normal finding. In absence of a seashore sign or presence of a stratosphere sign, pneumothorax is likely. B-lines or "comet trails" are echogenic bright linear reflections beneath the pleura that are usually lost with any air between the probe and the lung tissue and therefore whose presence with seashore sign indicates absence of a pneumothorax.[6][8]
Sinusoid sign is another M-mode finding indicating presence of pleural effusion. Due to the cyclical movement of the lung in inspiration and expiration, the motion-time tracing (M-mode) ultrasound shows a sinusoid appearance between the fluid and the line tissue. This finding indicates a possible pleural effusion, empyema, blood in pleural space (hemothorax).[6][7]
Advantages
FAST is less invasive than diagnostic peritoneal lavage, involves no exposure to radiation and is cheaper compared to computed tomography, but achieves a similar accuracy.[9]
Numerous studies have shown FAST is useful in evaluating trauma patients.[10][11][12][13] It also appears to make emergency department care faster and better.[14][15]
Interpretation
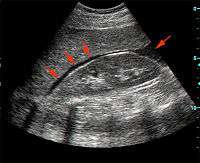
FAST is most useful in trauma patients who are hemodynamically unstable. A positive FAST result is defined as the appearance of a dark ("anechoic") strip in the dependent areas of the peritoneum. In the right upper quadrant this typically appears in Morison's Pouch (between the liver and kidney). This location is most useful as it is the place where fluid will collect with a supine patient. In the left upper quadrant, blood may collect anywhere around the spleen (perisplenic space). In the pelvis, blood generally pools behind the bladder (in the rectovesicular space). A positive result suggests hemoperitoneum; often CT scan will be performed if the patient is stable[17] or a laparotomy if unstable. In those with a negative FAST result, a search for extra-abdominal sources of bleeding may still need to be performed.
See also
References
- http://www.sonoguide.com/FAST.html
- Kirkpatrick AW, Sirois M, Laupland KB, et al., J Trauma, 2004;57(2):288–95.
- Zhang M, Liu ZH, Yang JX, et al., Crit Care, 2006;10(4):R112.
- Blaivas M, Lyon M, Duggal SA, Acad Emerg Med, 2005;12(9):844–9.
- Davis JA, et al. Critical Diagnosis in Bedside Ultrasonography. Diagnostics & Imaging. 2007.
- Christopher P. Holstege; Alexander B. Baer; Jesse M. Pines; William J. Brady (2011). Visual Diagnosis in Emergency and Critical Care Medicine. Wiley-Blackwell. pp. 95–7.
- Christoph T. Bolliger; F. J. F. Herth; P. Mayo; T. Miyazawa; J. Beamis (2009). Clinical chest ultrasound: from the ICU to the bronchoscopy suite. Karger Publishers. pp. 86–8.
- Steven G. Rothrock (M.D.) (2009). Tarascon Adult Emergency Pocketbook. Tarascon. p. 144.
- Rozycki G, Shackford S (1996). "Ultrasound, what every trauma surgeon should know". J Trauma. 40 (1): 1–4. doi:10.1097/00005373-199601000-00001. PMID 8576968.
- Dolich MO, McKenney MG, Varela JE, Compton RP, McKenney KL, Cohn SM (Jan 2001). "2,576 ultrasounds for blunt abdominal trauma". Journal of Trauma. 50 (1): 108–12. doi:10.1097/00005373-200101000-00019. PMID 11231679.
- Farahmand N, Sirlin CB, Brown MA, Shragg GP, Fortlage D, Hoyt DB, Casola G (May 2005). "Hypotensive patients with blunt abdominal trauma: performance of screening US". Radiology. 235 (2): 436–43. doi:10.1148/radiol.2352040583. PMID 15798158.
- Sirlin CB, Brown MA, Andrade-Barreto OA, Deutsch R, Fortlage DA, Hoyt DB, Casola G (Mar 2004). "Blunt abdominal trauma: clinical value of negative screening US scans". Radiology. 230 (3): 661–8. doi:10.1148/radiol.2303021707. PMID 14990832.
- Moylan M, Newgard CD, Ma OJ, Sabbaj A, Rogers T, Douglass R (Oct 2007). "Association between a positive ED FAST examination and therapeutic laparotomy in normotensive blunt trauma patients". Journal of Emergency Medicine. 33 (3): 265–71. doi:10.1016/j.jemermed.2007.02.030. PMID 17976554.
- Melniker LA, Leibner E, McKenney MG, Lopez P, Briggs WM, Mancuso CA (Sep 2006). "Randomized controlled clinical trial of point-of-care, limited ultrasonography for trauma in the emergency department: the first sonography outcomes assessment program trial". Annals of Emergency Medicine. 48 (3): 227–35. doi:10.1016/j.annemergmed.2006.01.008. PMID 16934640.
- Ollerton JE, Sugrue M, Balogh Z, D'Amours SK, Giles A, Wyllie P (Apr 2006). "Prospective study to evaluate the influence of FAST on trauma patient management". Journal of Trauma. 60 (4): 785–91. doi:10.1097/01.ta.0000214583.21492.e8. PMID 16612298.
- "UOTW #18 - Ultrasound of the Week". Ultrasound of the Week. 17 September 2014. Retrieved 27 May 2017.
- Scalea T, Rodriguez A, Chiu W, Brenneman F, Fallon W, Kato K, McKenney M, Nerlich M, Ochsner M, Yoshii H (1999). "Focused Assessment with Sonography for Trauma (FAST): results from an international consensus conference". Journal of Trauma. 46 (3): 466–72. doi:10.1097/00005373-199903000-00022. PMID 10088853.
- Further reading
- Gillman, Lawrence M; Ball, Chad G; Panebianco, Nova; Al-Kadi, Azzam; Kirkpatrick, Andrew W (2009). "Clinician performed resuscitative ultrasonography for the initial evaluation and resuscitation of trauma". Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 17 (1): 34. doi:10.1186/1757-7241-17-34. PMC 2734531.
External links
- Focus On: EFAST - Extended Focused Assessment With Sonography for Trauma: American College of Emergency Physicians (ACEP)
- eMedicine: Blunt abdominal trauma
- FAST exam tutorial
- The FAST examination from Trauma.org, includes tutorial videos.
- Trauma FAST Exam - LUQ Exam
- Lung ultrasound: ICU Sonography
- FOB Doc: Capt Ray Wiss, MD. By a pioneering teacher of FAST to ER and first responders, civilian and military.
| X-ray/ Radiography |
| ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MRI | |||||||||||||
| Ultrasound | |||||||||||||
| Radionuclide |
| ||||||||||||
| Optical/Laser | |||||||||||||
| Thermography |
| ||||||||||||
| Target conditions |
| ||||||||||||
| |||||||||||||