Electric acoustic stimulation
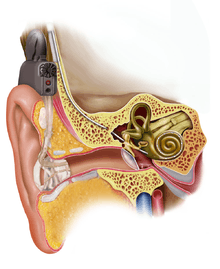
Electric acoustic stimulation (EAS) is the use of a hearing aid and a cochlear implant together in the same ear. The hearing aid acoustically amplifies low frequencies, while the cochlear implant electrically stimulates the middle and high frequencies. The inner ear processes acoustic and electric stimuli simultaneously.
The results of international studies have shown a highly synergistic effect between hearing aid and cochlear implant technology, particularly evident in speech understanding in noise, pitch discrimination and music appreciation.
Introduction
Electric stimulation of the auditory system via cochlear implant is a commonly used technique for individuals with a severe to profound sensorineural hearing loss, as well as for those adults and children with some residual hearing.
Individuals suffering from mild to moderate hearing loss can usually benefit from hearing aids. This acoustic stimulation proves to be particularly effective in the low frequencies, though a severe hearing loss (> 70 dB HL) above 1 kHz can be beyond the range of amplification possible via acoustic stimulation. Electric stimulation (CI), on the other hand, is capable of providing high-frequency information up to 8 kHz.
The concept of combining simultaneous electric-acoustic stimulation (EAS) for the purposes of better hearing was first described by C. von Ilberg and J. Kiefer, from the Universitätsklinik Frankfurt, Germany, in 1999. That same year the first EAS patient was implanted.
Indications
There is a certain patient group that has some degree of residual hearing in the low frequencies and a severe hearing loss in the high frequencies. This group only receives limited benefits from traditional amplification because of the severity of the hearing loss in the high frequencies. They suffer from inadequate speech comprehension, even in the best aided condition. Nor are they classic cochlear implant candidates, because of their mostly intact low frequency residual hearing.
The indications for EAS are based on the following three considerations:
- Audiogram
- Speech scores
- Additional selection criteria
Audiogram
below 1.5 kHz – No or moderate HL
above 1.5 kHz – Severe to profound sensorineural hearing impairment
Speech scores
The patient's monosyllable word score should be ≤ 60% at 65 dB SPL in the best aided condition.
Additional selection criteria
Contraindicated are:
- Progressive hearing loss
- Autoimmune disease
- Hearing loss as a result of meningitis, otosclerosis or ossification
- Malformation or obstruction of the cochlea
- Air–bone gap > 15 dB HL
- External ear contra-indications to using amplification devices
Hearing preservation surgery
A special surgical technique is the key to preserving the residual hearing of the patient. In most routine cochlear implant surgeries, any residual hearing will likely be destroyed.
Important factors for preserving residual hearing are:
- Special atraumatic soft electrodes
- Smallest possible acoustic trauma due to cochleostomy drilling
- Smallest possible mechanical trauma due to drilling and electrode insertion
- Avoidance of inflammatory and fibrotic reactions (contamination with blood, bone dust, middle ear bacteria, etc.)
- The use of drugs that will aid in the preservation of hearing
Two methods are commonly used for inserting the electrode into the cochlea:
- Round-window insertion
- Cochleostomy insertion
Most recently, round-window insertion has found a wider acceptance because it is considered to be less traumatic. The best results have been achieved with electrode insertion depths of 18 mm, which corresponds to the approximate place in the normal sized cochlea where 1000 Hz is processed. As a result, frequencies below 1000 Hz are stimulated acoustically, and above 1000 Hz are stimulated electrically.
For those interested in gaining the latest expertise necessary for a successful treatment of EAS candidates, surgical and professional training courses are provided by companies that offer EAS products.
EAS electrodes for cochlear implants
Long-term research has shown that mechanical flexibility of the electrode array is one of the key factors for preserving residual hearing. The smaller the force used to insert the electrode, the greater the chance of protecting the fragile structures within the cochlea.
Today only lateral wall electrodes are used. Studies with preshaped (modiolus-hugging electrodes) have been proven to be not so effective.
Studies with different lengths of electrodes have shown that an insertion depth of 10 mm has a good chance of preserving residual hearing but on the other hand yields little benefit in speech understanding in comparison to the hearing aid only condition. Electrodes that can be inserted to a depth of 18–22 mm are a good compromise. The insertion depth also depends on the size of the cochlea of the patient, though a range of 18–22 mm can be used as a general rule of thumb for insertion in most cochleas.
EAS audio processors

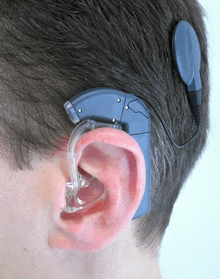
Several devices are under investigation; however there is only one approved device currently available that combines cochlear implant technology with a digital hearing aid. This device uses one microphone for the input, but has two separate digital sound processors for differentiated processing.
The parallel processing of these signals, however, is performed separately and optimized for both acoustic hearing (focusing on low-frequency hearing) and cochlear implant stimulation (focusing on high-frequency hearing). The hearing aid is integrated in the ear hook and the amplified signals are forwarded to the auditory pathway via an ear mould. The ear mould used for the acoustic component is similar to a conventional hearing aid ear mould and can be exchanged.
See also
External links
References
- V. Ilberg C., Kiefer J., Tillein J., Pfennigdorff T., Hartmann R., Stürzebecher E., Klinke R. (1999).Electric-acoustic stimulation of the auditory system. ORL 61:334–340.
- Skarzynski H, Lorens A, Piotrowska A, Anderson I (2006). Partial deafness cochlear implantation provides benefit to a new population of individuals with hearing loss Acta Otolaryngol. 2006, Vol. 126/9: 934–40.
- Gstoettner W., Helbig S., Maier N., Kiefer J., Radeloff A., Adunka O. (2006). Ipsilateral Electric Acoustic Stimulation of the Auditory System: Results of Long-Term Hearing Preservation. Audiology & Neurotology: 11 (suppl 1): 49–56.