Desmoplastic small-round-cell tumor
Desmoplastic small-round-cell tumor (DSRCT) is an aggressive and rare cancer that primarily occurs as masses in the abdomen.[2] Other areas affected may include the lymph nodes, the lining of the abdomen, diaphragm, spleen, liver, chest wall, skull, spinal cord, large intestine, small intestine, bladder, brain, lungs, testicles, ovaries, and the pelvis. Reported sites of metastatic spread include the liver, lungs, lymph nodes, brain, skull, and bones.
| Desmoplastic small-round-cell tumor | |
|---|---|
| Other names | DSRCT[1] |
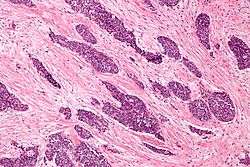 | |
| Micrograph of a desmoplastic small round cell tumor, showing the characteristic desmoplastic stroma and angulated nests of small round cells. H&E stain. | |
| Specialty | Oncology |
The tumor is classified as a soft tissue sarcoma. It is considered a childhood cancer that predominantly strikes boys and young adults. The disease rarely occurs in females, but when it does the tumors can be mistaken for ovarian cancer.[3]
In dogs, mast cell tumors are the most frequent round-cell tumor.[4]
Signs and symptoms
There are few early warning signs that a patient has a DSRCT. Patients are often young and healthy as the tumors grow and spread uninhibited within the abdominal cavity. These are rare tumors and symptoms are often misdiagnosed by physicians. The abdominal masses can grow to enormous size before being noticed by the patient. The tumors can be felt as hard, round masses by palpating the abdomen.
First symptoms of the disease often include abdominal distention, abdominal mass, abdominal or back pain, gastrointestinal obstruction, lack of appetite, ascites, anemia, and cachexia.
Other reported symptoms include unknown lumps, thyroid conditions, hormonal conditions, blood clotting, kidney and urological problems, testicle, breast, uterine, vaginal, and ovarian masses.
Causes
There are no known risk factors that have been identified specific to the disease. The tumor appears to arise from the primitive cells of childhood, and is considered a childhood cancer.
Research has indicated that there is a chimeric relationship between DSRCT and Wilms' tumor and Ewing's sarcoma. Together with neuroblastoma and non-Hodgkin's lymphoma, they form the small-cell tumors.
DSRCT is associated with a unique chromosomal translocation t(11;22)(p13:q12)[5] resulting in an EWS/WT1 transcript[6] that is diagnostic of this tumor.[7] This transcript codes for a protein that acts as a transcriptional activator that fails to suppress tumor growth.
The EWS/WT1 translocation product targets ENT4.[8] ENT4 is also known as PMAT.
Pathology
The entity was first described by pathologists William L. Gerald and Juan Rosai in 1989.[9] Pathology reveals well circumscribed solid tumor nodules within a dense desmoplastic stroma. Often areas of central necrosis are present. Tumor cells have hyperchromatic nuclei with increased nuclear/cytoplasmic ratio.
On immunohistochemistry, these cells have trilinear coexpression including the epithelial marker cytokeratin, the mesenchymal markers desmin and vimentin, and the neuronal marker neuron-specific enolase. Thus, although initially thought to be of mesothelial origin due to sites of presentation, it is now hypothesized to arise from a progenitor cell with multiphenotypic differentiation.
Diagnosis
Differential diagnosis
Because this is a rare tumor, not many family physicians or oncologists are familiar with this disease. DSRCT in young patients can be mistaken for other abdominal tumors including rhabdomyosarcoma, neuroblastoma, and mesenteric carcinoid. In older patients DSRCT can resemble lymphoma, peritoneal mesothelioma, and peritoneal carcinomatosis. In males DSRCT may be mistaken for germ cell or testicular cancer while in females DSRCT can be mistaken for Ovarian cancer. DSRCT shares characteristics with other small-round blue cell cancers including Ewing's sarcoma, acute leukemia, small cell mesothelioma, neuroblastoma, primitive neuroectodermal tumor, rhabdomyosarcoma, and Wilms' tumor.
Treatment
DSRCT is frequently misdiagnosed. Adult patients should always be referred to a sarcoma specialist. This is an aggressive, rare, fast spreading tumor and both pediatric and adult patients should be treated at a sarcoma center.
There is no standard protocol for the disease;[10] however, recent journals and studies have reported that some patients respond to high-dose (P6 Protocol) chemotherapy, maintenance chemotherapy, debulking operation, cytoreductive surgery, and radiation therapy. Other treatment options include: hematopoietic stem cell transplantation, intensity-modulated radiation therapy, radiofrequency ablation, stereotactic body radiation therapy, intraperitoneal hyperthermic chemoperfusion, and clinical trials.
Prognosis
The prognosis for DSRCT remains poor.[11] Prognosis depends upon the stage of the cancer. Because the disease can be misdiagnosed or remain undetected, tumors frequently grow large within the abdomen and metastasize or seed to other parts of the body.
There is no known organ or area of origin. DSRCT can metastasize through lymph nodes or the blood stream. Sites of metastasis include the spleen, diaphragm, liver, large and small intestine, lungs, central nervous system, bones, uterus, bladder, genitals, abdominal cavity, and the brain.
A multi-modality approach of high-dose chemotherapy, aggressive surgical resection,[12] radiation, and stem cell rescue improves survival for some patients. Reports have indicated that patients will initially respond to first line chemotherapy and treatment but that relapse is common.
Some patients in remission or with inoperable tumor seem to benefit from long term low dose chemotherapy, turning DSRCT into a chronic disease.
Research
The Stehlin Foundation[13] currently offers DSRCT patients the opportunity to send samples of their tumors free of charge for testing. Research scientists are growing the samples on nude mice and testing various chemical agents to find which are most effective against the individual's tumor.
Patients with advanced DSRCT may qualify to participate in clinical trials that are researching new drugs to treat the disease.
The Cory Monzingo Foundation is a 501(c)(3) organization that supports the research for treatments and a cure for DSRCT. The Cory Monzingo Foundation provides funding to MD Anderson Cancer Center and may also provide funding to other nonprofit cancer research organizations.
In 2002, Nishio and al[14], established a novel human tumor cell line derived from the pleural effusion of a patient with a typical intra-abdominal DSRCT, called JN-DSRCT-1[15] that can now be used in research.
St. Jude Children’s Research Hospital has, in 2018, make available resources from the Childhood Solid Tumor Network, that upon request gives access to patient-derived orthotopic xenografts[16].
Alternative names
This disease is also known as: desmoplastic small round blue cell tumor; intra-abdominal desmoplastic small round blue cell tumor; desmoplastic small cell tumor; desmoplastic cancer; desmoplastic sarcoma; DSRCT.
There is no connection to peritoneal mesothelioma which is another disease sometimes described as desmoplastic.
See also
- Kate Granger (1981–2016), an English physician, whose diagnosis with DSRCT led to her campaigning for better patient care, and fund-raising for cancer research.
References
- RESERVED, INSERM US14-- ALL RIGHTS. "Orphanet: Desmoplastic small round cell tumor". www.orpha.net. Retrieved 17 November 2019.
- Lee YS, Hsiao CH: Desmoplastic small round cell tumor: a clinicopathologic, immunohistochemical and molecular study of four patients. J Formos Med Assoc 2007; 106: 854–860.
- Bland AE, Shah AA, Piscitelli JT, Bentley RC, Secord AA (2007). "Desmoplastic small round cell tumor masquerading as advanced ovarian cancer". Int J Gynecol Cancer. 18 (4): 847–50. doi:10.1111/j.1525-1438.2007.01110.x. PMID 18081791.
- Mackowiak II et al. (2012) E-cadherin in canine mast cell tumors: Decreased expression and altered subcellular localization in Grade 3 tumors. Vet J 194(3):405-11
- Murphy AJ, Bishop K, Pereira C, et al. (December 2008). "A new molecular variant of desmoplastic small round cell tumor: significance of WT1 immunostaining in this entity". Hum. Pathol. 39 (12): 1763–70. doi:10.1016/j.humpath.2008.04.019. PMID 18703217.
- Gerald WL, Haber DA (June 2005). "The EWS-WT1 gene fusion in desmoplastic small round cell tumor". Semin. Cancer Biol. 15 (3): 197–205. doi:10.1016/j.semcancer.2005.01.005. PMID 15826834.
- Lee YS, Hsiao CH (2007). "Desmoplastic small round cell tumor: a clinicopathologic, immunohistochemical and molecular study of four patients". J. Formos. Med. Assoc. 106 (10): 854–60. doi:10.1016/S0929-6646(08)60051-0. PMID 17964965.
- Li H, Smolen GA, Beers LF, et al. (2008). "Adenosine transporter ENT4 is a direct target of EWS/WT1 translocation product and is highly expressed in desmoplastic small round cell tumor". PLoS ONE. 3 (6): e2353. Bibcode:2008PLoSO...3.2353L. doi:10.1371/journal.pone.0002353. PMC 2394657. PMID 18523561.

- Gerald, W. L.; Rosai, J. (1989). "Case 2. Desmoplastic small cell tumor with divergent differentiation". Pediatr. Pathol. 9 (2): 177–83. doi:10.3109/15513818909022347. PMID 2473463.
- Talarico F, Iusco D, Negri L, Belinelli D: Combined resection and multi-agent adjuvant chemotherapy for intra-abdominal desmoplastic small round cell tumour: case report and review of the literature. G Chir 2007; 28: 367–370.
- Lal DR, Su WT, Wolden SL, Loh KC, Modak S, La Quaglia MP (January 2005). "Results of multimodal treatment for desmoplastic small round cell tumors". J. Pediatr. Surg. 40 (1): 251–5. doi:10.1016/j.jpedsurg.2004.09.046. PMID 15868593.
- Talarico F, Iusco D, Negri L, Belinelli D (October 2007). "Combined resection and multi-agent adjuvant chemotherapy for intra-abdominal desmoplastic small round cell tumour: case report and review of the literature". G Chir. 28 (10): 367–70. PMID 17915050.
- Official website for Stehlin Foundation
- Nishio, Jun; Iwasaki, Hiroshi; Ishiguro, Masako; Ohjimi, Yuko; Fujita, Chikako; Yanai, Fumio; Nibu, Keiko; Mitsudome, Akihisa; Kaneko, Yasuhiko (September 2002). "Establishment and characterization of a novel human desmoplastic small round cell tumor cell line, JN-DSRCT-1". Laboratory Investigation; A Journal of Technical Methods and Pathology. 82 (9): 1175–1182. doi:10.1097/01.LAB.0000028059.92642.03. ISSN 0023-6837. PMID 12218078.
- "Jn-Dsrct-1".
- "St Jude Children's Research Hospital".