Cutis marmorata telangiectatica congenita
Cutis marmorata telangiectatica congenita is a rare congenital vascular disorder that usually manifests in affecting the blood vessels of the skin. The condition was first recognised and described in 1922 by Cato van Lohuizen,[3] a Dutch pediatrician whose name was later adopted in the other common name used to describe the condition – Van Lohuizen Syndrome. CMTC is also used synonymously with congenital generalized phlebectasia, nevus vascularis reticularis, congenital phlebectasia, livedo telangiectatica, congenital livedo reticularis and Van Lohuizen syndrome.[4]
| Cutis marmorata telangiectatica congenita | |
|---|---|
| Other names | CMTC[1] |
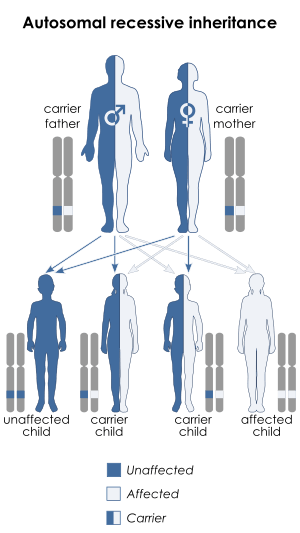 | |
| Cutis marmorata telangiectatica congenital is inherited via autosomal recessive manner[2] | |
| Specialty | Dermatology |
It should not be confused with the more general term "cutis marmorata", which refers to livedo reticularis caused by cold.[5]
Signs and symptoms
People with visible marks generally feel fine (physically) and can act normally, but when it is mentioned, they may become withdrawn and self-conscious. Some children may have low self-esteem due to the condition.
CMTC is an uncommon, sporadic congenital vascular malformation characterized by a generalized or localized reticulated cutaneous vascular network.
Cutaneous lesions described in patients with CMTC include nevus flammeus, hemangioma, nevus anemicus, café-au-lait spots, melanocytic nevus, aplasia cutis and acral cyanosis.[6]
It has a marbled bluish to deep-purple appearance. The dark skin lesions often show a palpable loss of dermal substance. The reticulated mottling frequently appears more prominent in a cold environment (physiologic cutis marmorata), but tends not to disappear with warming. Hence, the erythema may be worsened by cooling, physical activity, or crying.
CMTC frequently involves the extremities, with the lower extremities involved most commonly, followed by the upper extremities, and then the trunk and face. The lower extremities often show atrophy and seldom show hypertrophy resulting in limb circumference discrepancy.
When located on the trunk, the lesions of CMTC tend to show mosaic distribution in streaks with a sharp midline demarcation seen across the abdomen.[6] The lesions are primarily localized, but can be segmental or generalized, often unilateral in appearance.[6] Diffuse involvement of the skin is usually not observed.
Although its course is variable, the majority of lesions in mild cases fade by adolescence. Ulceration and secondary infection are complications in severe cases and can be fatal if present in the neonatal period.[7]
Causes
Fewer than 100 cases of CMTC have been published worldwide. Petrozzi reported the first case of CMTC in the United States in 1970.[8] CMTC is believed to be more common than suspected, as studies have shown that milder forms of the disease are not being recognized as CMTC.[6]
The pathophysiology is still unclear, with most cases occurring sporadically, although rare cases were reported in families. Studies indicated the primary involvement of capillaries, venules and veins, and possibly also that of arterioles and lymphatics.
Hypotheses that have been proposed include: environmental/external factors;[9] peripheral neural dysfunction;[10] failure of the development of mesodermic vessels in an early embryonic stage; autosomal dominant inheritance with incomplete penetrance and, finally, the theory of Happle.[10]
Diagnosis
Differential diagnosis
During the first few weeks after birth, when the lesions are not very reticulated, CMTC may look very similar to vascular lesions such as port-wine stains. However, during follow-up, CMTC lesions become characteristic in their appearance. They must be differentiated from other causes of persistent reticulated vascular lesions, such as those in the following table:
| Diseases | Characteristics |
|---|---|
| Diffuse phlebectasia | rare progressive harmartomatous malformation involving the deeper veins |
| Livedo reticularis associated with collagen-vascular disease | lace pattern of cyanotic skin discoloration secondary to dilation of subpapillary veinous plexi and occlusion of small vessels feeding the upper cutis |
| Neonatal lupus erythematosus | well-demarcated erythematous, mild-scaling plaque that is often annular and appears predominantly on the scalp, neck, or face |
| Nevus anemicus | congenital single patch manifested by skin pallor, most commonly seen on the trunk |
| Nevus flammeus (port-wine stain) | pale pink to red-purple, usually unilateral macules of the face or extremities |
| Physiologic cutis marmorata | reticulated mottling appearance of the skin that physiologically responds to cold environments |
| Primary antiphospholipid syndrome (APS) | increased tendency to form venous and/or arterial thromboses, often accompanied by thrombocytopenia in the presence of the antiphospholipid antibodies |
Histology
Some patients have a few or no histopathologic abnormalities. Histological examination of a biopsy may show an increase in the number and size of capillaries and veins (rarely lymphatics), dilated capillaries located in the deeper dermis, and hyperplasia and swollen endothelial cells with occasional dilated veins and venous lakes.
Associated abnormalities
Associated abnormalities include the following: • Body asymmetry (extremities; macrocephaly) • Glaucoma • Cutaneous atrophy • Neurological anomalies • Vascular anomalies (nevus flammeus /Sturge-Weber/Klippel-Trénauna Adams Oliver syndrome) • Psychomotor and/or mental retardation • Chronic ulceration that can complicate long-term CMTC • Chronic urticaria.[11]
Treatment
In general, there is no treatment available for CMTC, although associated abnormalities can be treated. In the case of limb asymmetry, when no functional problems are noted, treatment is not warranted, except for an elevation device for the shorter leg.
Laser therapy has not been successful in the treatment of CMTC, possibly due to the presence of many large and deep capillaries and dilated veins. Pulsed-dye laser and long-pulsed-dye laser have not yet been evaluated in CMTC, but neither argon laser therapy nor YAG laser therapy has been helpful.[12]
When ulcers develop secondary to the congenital disease, antibiotic treatment such as oxacillin and gentamicin administered for 10 days has been prescribed. In one study, the wound grew Escherichia coli while blood cultures were negative.[7]
Prognosis
The prognosis is favorable in most patients with an isolated cutaneous abnormality. In the majority of cases, both the vivid red marking and the difference in circumference of the extremities regress spontaneously during the first year of life. It is theorized that this may be due to the normal maturation process, with thickening of the epidermis and dermis. Improvements for some patients can continue for up to 10 years, while in other cases, the marbled skin may persist for the patient's lifetime.
One study reported an improvement in lesions in 46% of patients within 3 years.[9] If CMTC persists into adulthood, it can result in complaints due to paresthesia, increased sensitivity to cold and pain, and the formation of ulcers.[7]
Few reports included long-term follow up of CMTC into adolescence and adulthood. While about 50% of patients seem to show definite improvement in the reticular vascular pattern,[12] the exact incidence and cause of persistent cases are unknown.
Epidemiology
Usually observed at birth or shortly thereafter in 94% of patients,[9] in other reports, patients did not develop skin lesions until 3 months or even 2 years after birth.[13][14] Females are typically affected more often than males (64%).[15]
Eponym
It is named for Dr. Cato van Lohuizen.[16]
References
- RESERVED, INSERM US14-- ALL RIGHTS. "Orphanet: Cutis marmorata telangiectatica congenita". www.orpha.net. Retrieved 28 April 2019.
- "OMIM Entry – 219250 – CUTIS MARMORATA TELANGIECTATICA CONGENITA; CMTC". omim.org. Retrieved 10 July 2017.
- Van Lohuizen CHJ. Cutis marmorata telangiectatica congenita,. Acta Derm Venereol. (Stockh). 1922:3:202-11.
- Gerritsen MJ, et al. Cutis marmorata telangiectatica congenita: report of 18 cases. Br J Dermatol. 2000 Feb;142(2):366-9.
- "cutis marmorata" at Dorland's Medical Dictionary
- Torrelo A, Zambrano A, Happle R. Cutis marmorata telangiectatica congenita and extensive mongolian spots: type 5 phacomatosis pigmentovascularis. Br J Dermatol. 2003 Feb;148(2):342-5.
- Hu IJ, Chen MT, Tai HC, et al. Cutis marmorata telangiectatica congenita with gangrenous ulceration and hypovolaemic shock. Eur J Pediatr. 2005 Jul;164(7):411-3.
- Petrozzi JW, Rahn EK, Mofenson H, et al. Cutis marmorata telangiectatica congenita. Arch Dermatol. 1970 Jan;101(1):74-7.
- Amitai DB, Fichman S, Merlob P, et al. Cutis marmorata telangiectatica congenita: clinical findings in 85 patients. Ped Dermatol. 2000 Mar–Apr;17(2):100-4.
- Bormann G, Wohlrab J, Fischer M, et al. Cutis marmorata telangiectatica congenita: laser doppler fluxmetry evidence for a functional nervous defect. Ped Dermatol. 2001Mar-Apr;18(2):110-3.
- Melani L, Antiga E, Torchia D, et al. Cutis marmorata telangiectatica congenita and chronic autoimmune urticaria in a young man. J Dermatol. 2007 Mar;34(3):210-3.
- Mazereeuw-Hautier J, Carel-Caneppele S, Bonafe JL. Cutis marmorata telangiectatica congenita: report of two persistent cases. Ped Dermatol. 2002 Nov–Dec;19(6): 506–9.
- Powel ST, Su WP. Cutis marmorata telangiectatica congenita: report of nine cases and review of the literature. Cutis. 1984 Sep;34(3):305-12. Review.
- Lee S, Lee JB, Kim JH, et al. Cutis marmorata telangiectatica congenita with multiple congenital anomalies (van Lohuizen’s syndrome). Dermatologica. 1981;163(5):408-12.
- Vascular Lesions and Congenital Nevi in the Newborn. UpToDate viewed on 03-28-2008. http://www.utdol.com/utd/content/topic.do?topicKey=ped_derm/4439&type=P&selectedTitle=1~1%5B%5D.
- doctor/3295 at Who Named It?
External links
| Classification | |
|---|---|
| External resources |
|