Cryptogenic organizing pneumonia
Cryptogenic organizing pneumonia (COP), formerly known as bronchiolitis obliterans organizing pneumonia (BOOP), is an inflammation of the bronchioles (bronchiolitis) and surrounding tissue in the lungs).[1][2] It should not be confused with bronchiolitis obliterans, a form of non-infectious pneumonia.
| Cryptogenic organizing pneumonia | |
|---|---|
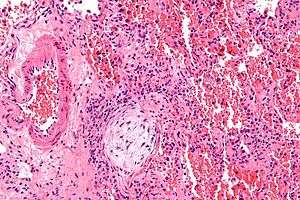 | |
| Micrograph showing a Masson body (off center left/bottom of the image – pale circular and paucicellular), as may be seen in cryptogenic organizing pneumonia. The Masson body plugs the airway. The artery associated with the obliterated airway is also seen (far left of the image). H&E stain. | |
| Specialty | Pulmonology |
It is often a complication of an existing chronic inflammatory disease such as rheumatoid arthritis, dermatomyositis, or it can be a side effect of certain medications such as amiodarone. COP was first described by Gary Epler in 1985.[3]
The clinical features and radiological imaging resemble infectious pneumonia. However, diagnosis is suspected after there is no response to multiple antibiotics, and blood and sputum cultures are negative for organisms.
Terminology
"Organizing" refers to unresolved pneumonia (in which the alveolar exudate persists and eventually undergoes fibrosis) in which fibrous tissue forms in the alveoli. The phase of resolution and/or remodeling following bacterial infections is commonly referred to as organizing pneumonia, both clinically and pathologically.
The American Thoracic Society and the European Respiratory Society hold that "cryptogenic organizing pneumonia" is the preferred clinical term for this disease for multiple reasons:[4][5]
- Avoid confusion with bronchiolitis obliterans, which may not be visualized in every case of this disease.
- Avoid confusion with constrictive bronchiolitis
- Emphasize the cryptogenic nature of the disease
Signs and symptoms
The classic presentation of COP is the development of nonspecific systemic (e.g., fevers, chills, night sweats, fatigue, weight loss) and respiratory (e.g. difficulty breathing, cough) symptoms in association with filling of the lung alveoli that is visible on chest x-ray.[6] This presentation is usually so suggestive of an infection that the majority of patients with COP have been treated with at least one failed course of antibiotics by the time the true diagnosis is made.[6]
Causes
- Pulmonary infection by bacteria, viruses and parasites
- Drugs: antineoplastic drugs, erlotinib, amiodarone
- Chemical exposure, most notably to diacetyl[7]
- Ionizing radiations[9][10]
- Inflammatory diseases
- Systemic lupus
- Rheumatoid arthritis (RA-associated COP)
- Scleroderma
- Bronchial obstruction
It was identified in 1985, although its symptoms had been noted before but not recognised as a separate lung disease. The risk of COP is higher for people with inflammatory diseases like lupus, dermatomyositis, rheumatoid arthritis, and scleroderma.[12]
Diagnosis
On clinical examination, crackles are common, and more rarely, patients may have clubbing (<5% of cases). Laboratory findings are nonspecific.
Almost 75% of people have symptoms for less than two months before seeking medical attention. A flu-like illness, with a cough, fever, a feeling of illness (malaise), fatigue, and weight loss heralds the onset in about 40% of patients. Doctors do not find any specific abnormalities on routine laboratory tests or on a physical examination, except for the frequent presence of crackling sounds (called rales) upon auscultation with a stethoscope by the care provider. Pulmonary function tests usually show that the amount of air the lungs can hold is below normal. The amount of oxygen in the blood is often low at rest and is even lower with exercise.
Imaging

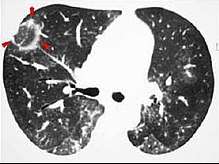
The chest x-ray is distinctive with features that appear similar to an extensive pneumonia, with both lungs showing widespread white patches. The white patches may seem to migrate from one area of the lung to another as the disease persists or progresses. Computed tomography (CT) may be used to confirm the diagnosis. Often the findings are typical enough to allow the doctor to make a diagnosis without ordering additional tests.[14] To confirm the diagnosis, a doctor may perform a lung biopsy using a bronchoscope. Many times, a larger specimen is needed and must be removed surgically.
Plain chest radiography shows normal lung volumes, with characteristic patchy unilateral or bilateral consolidation. Small nodular opacities occur in up to 50% of patients and large nodules in 15%. On high resolution computed tomography, airspace consolidation with air bronchograms is present in more than 90% of patients, often with a lower zone predominance. A subpleural or peribronchiolar distribution is noted in up to 50% of patients. Ground glass appearance or hazy opacities associated with the consolidation are detected in most patients.
Pulmonary physiology is restrictive with a reduced diffusion capacity of the lung for carbon monoxide (DLCO). Airflow limitation is uncommon; gas exchange is usually abnormal and mild hypoxemia is common. Bronchoscopy with bronchoalveolar lavage reveals up to 40% lymphocytes, along with more subtle increases in neutrophils and eosinophils. In patients with typical clinical and radiographic features, a transbronchial biopsy that shows the pathologic pattern of organizing pneumonia and lacks features of an alternative diagnosis is adequate to make a tentative diagnosis and start therapy. On surgical lung biopsy, the histopathologic pattern is organizing pneumonia with preserved lung architecture; this pattern is not exclusive to COP and must be interpreted in the clinical context.
Histologically, cryptogenic organizing pneumonia is characterized by the presence of polypoid plugs of loose organizing connective tissue (Masson bodies) within alveolar ducts, alveoli, and bronchioles.
Unusual presentations of organizing pneumonia
While patchy bilateral disease is typical, there are unusual variants of organizing pneumonia where it may appear as multiple nodules or masses. One rare presentation, focal organizing pneumonia, may be indistinguishable from lung cancer based on imaging alone, requiring biopsy or surgical resection to make the diagnosis.[15]
Complications
Rare cases of COP have induced with lobar cicatricial atelectasis.[16]
Treatment
Most patients recover with corticosteroid therapy.[17] A standardized approach to dosing starting at 0.75 mg/kg and weaning over 24 weeks has been shown to reduce total corticosteroid exposure without affecting outcome.
About two thirds of patients recover with corticosteroid therapy: the usual corticosteroid administered is prednisolone in Europe and prednisone in the US; these differ by only one functional group and have the same clinical effect. The corticosteroid is initially administered in high dosage, typically 50 mg per day tapering down to zero over a six-month to one-year period. If the corticosteroid treatment is halted too quickly the disease may return.
References
- "bronchiolitis obliterans with organizing pneumonia" at Dorland's Medical Dictionary
- White, Eric J. Stern, Charles S. (1999). Chest radiology companion. Philadelphia: Lippincott Williams & Wilkins. p. 76. ISBN 978-0-397-51732-9.
- Epler GR (June 2011). "Bronchiolitis obliterans organizing pneumonia, 25 years: a variety of causes, but what are the treatment options?". Expert Rev Respir Med. 5 (3): 353–61. doi:10.1586/ers.11.19. PMID 21702658.
- [https://books.google.se/books?id=j-eYLc1BA3oC&pg=PA64 Page 64 in: Joseph F. Tomashefski, Carol Farver, Armando E. Fraire (2009). Dail and Hammar's Pulmonary Pathology: Volume I: Nonneoplastic Lung Disease (3 ed.). Springer Science & Business Media. ISBN 9780387687926.CS1 maint: multiple names: authors list (link)
- Geddes DM (August 1991). "BOOP and COP". Thorax. 46 (8): 545–7. doi:10.1136/thx.46.8.545. PMC 463266. PMID 1926020.
- "Pulmonary Question 27: Diagnose cryptogenic organizing pneumonia". MKSAP 5 For Students Online. American College of Physicians. Retrieved 23 November 2012.
- Levy, Barry S.; Wegman, David H.; Baron, Sherry L.; Sokas, Rosemary K., eds. (2011). Occupational and environmental health recognizing and preventing disease and injury (6th ed.). New York: Oxford University Press. p. 414. ISBN 9780199750061. Retrieved June 23, 2015.
- Mukhopadhyay, Sanjay; Mehrad, Mitra; Dammert, Pedro; Arrossi, Andrea V; Sarda, Rakesh; Brenner, David S; Maldonado, Fabien; Choi, Humberto; Ghobrial, Michael (2019). "Lung Biopsy Findings in Severe Pulmonary Illness Associated With E-Cigarette Use (Vaping): A Report of Eight Cases". American Journal of Clinical Pathology. doi:10.1093/ajcp/aqz182. ISSN 0002-9173.
- Nogi, S; Nakayama, H; Tajima, Y; Okubo, M; Mikami, R; Sugahara, S; Akata, S; Tokuuye, K (2014). "Cryptogenic organizing pneumonia associated with radiation: A report of two cases". Oncology Letters. 7 (2): 321–324. doi:10.3892/ol.2013.1716. PMC 3881924. PMID 24396439.
- Oie, Y; Saito, Y; Kato, M; Ito, F; Hattori, H; Toyama, H; Kobayashi, H; Katada, K (2013). "Relationship between radiation pneumonitis and organizing pneumonia after radiotherapy for breast cancer". Radiation Oncology. 8: 56. doi:10.1186/1748-717X-8-56. PMC 3605133. PMID 23497657.
- Radzikowska, E; Nowicka, U; Wiatr, E; Jakubowska, L; Langfort, R; Chabowski, M; Roszkowski, K (2007). "Organising pneumonia and lung cancer - case report and review of the literature". Pneumonologia i Alergologia Polska. 75 (4): 394–7. PMID 18080991.
- Al-Ghanem Sara; Al-Jahdali Hamdan; Bamefleh Hanaa; Khan Ali Nawaz (Apr–Jun 2008). "Bronchiolitis obliterans organizing pneumonia: Pathogenesis, clinical features, imaging and therapy review". Ann Thorac Med. 3 (2): 67–75. doi:10.4103/1817-1737.39641. PMC 2700454. PMID 19561910.
- Radswiki; et al. "Reversed halo sign (lungs)". Radiopaedia. Retrieved 2018-01-02.
- Zare Mehrjardi, Mohammad; Kahkouee, Shahram; Pourabdollah, Mihan (March 2017). "Radio-pathological correlation of organizing pneumonia (OP): a pictorial review". The British Journal of Radiology. 90 (1071): 20160723. doi:10.1259/bjr.20160723. ISSN 1748-880X. PMC 5601538. PMID 28106480.
- Oikonomou, A; Hansell, DM (2001). "Organizing pneumonia: the many morphological faces". European Radiology. 12 (6): 1486–96. doi:10.1007/s00330-001-1211-3. PMID 12042959.
- Yoshida, K; Nakajima, M; Niki, Y; Matsushima, T (2001). "Atelectasis of the right lower lobe in association with bronchiolitis obliterans organizing pneumonia". Nihon Kokyuki Gakkai zasshi = the journal of the Japanese Respiratory Society. 39 (4): 260–5. PMID 11481825.
- Oymak FS, Demirbaş HM, Mavili E, et al. (2005). "Bronchiolitis obliterans organizing pneumonia. Clinical and roentgenological features in 26 cases". Respiration. 72 (3): 254–62. doi:10.1159/000085366. PMID 15942294.
External links
| Classification | |
|---|---|
| External resources |
- "Idiopathic Interstitial Pneumonias". Merck Manual Professional. May 2008.