Cryptococcus neoformans
Cryptococcus neoformans is an encapsulated yeast[1] and an obligate aerobe[2] that can live in both plants and animals. Its teleomorph is Filobasidiella neoformans, a filamentous fungus belonging to the class Tremellomycetes. It is often found in bird excrement. Cryptococcus neoformans is an encapsulated fungal organism and it can cause disease in apparently immunocompetent, as well as immunocompromised, hosts.[3]
| Cryptococcus neoformans | |
|---|---|
 | |
| Cryptococcus neoformans | |
| Scientific classification | |
| Kingdom: | |
| Phylum: | Basidiomycota |
| Class: | Tremellomycetes |
| Order: | Tremellales |
| Family: | Tremellaceae |
| Genus: | |
| Species: | Cryptococcus neoformans |
| Binomial name | |
| Cryptococcus neoformans (San Felice) Vuill. | |
Classification
Cryptococcus neoformans has undergone numerous nomenclature revisions since its first description in 1894. For instance, it once contained two varieties (var.): C. neoformans var. neoformans and C. neoformans var. grubii. A third variety, C. neoformans var. gattii, was defined as a distinct species, Cryptococcus gattii. The most recent classification system divides organisms into seven species.[4] C. neoformans refers to C. neoformans var. grubii. A new species name, Cryptococcus deneoformans, is used for the former C. neoformans var. neoformans. C. gattii is divided into five species.
Characteristics

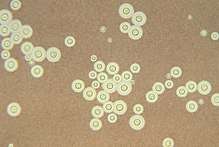
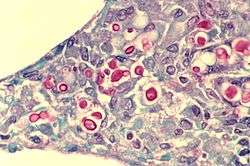
C. neoformans grows as a yeast (unicellular) and replicates by budding. It makes hyphae during mating, and eventually creates basidiospores at the end of the hyphae before producing spores. Under host-relevant conditions, including low glucose, serum, 5% carbon dioxide, and low iron, among others, the cells produce a characteristic polysaccharide capsule.[5] The recognition of C. neoformans in Gram-stained smears of purulent exudates may be hampered by the presence of the large gelatinous capsule which apparently prevents definitive staining of the yeast-like cells. In such stained preparations, it may appear either as round cells with Gram-positive granular inclusions impressed upon a pale lavender cytoplasmic background or as Gram-negative lipoid bodies.[6] When grown as a yeast, C. neoformans has a prominent capsule composed mostly of polysaccharides. Under the microscope, the India ink stain is used for easy visualization of the capsule in cerebral spinal fluid.[7] The particles of ink pigment do not enter the capsule that surrounds the spherical yeast cell, resulting in a zone of clearance or "halo" around the cells. This allows for quick and easy identification of C. neoformans. Unusual morphological forms are rarely seen.[8] For identification in tissue, mucicarmine stain provides specific staining of polysaccharide cell wall in C. neoformans. Cryptococcal antigen from cerebrospinal fluid is thought to be the best test for diagnosis of cryptococcal meningitis in terms of sensitivity, though it might be unreliable in HIV-positive patients.[9]
The first genome sequence for a strain of C. neoformans (var. neoformans; now C. deneoformans) was published in 2005.[10]
Studies suggest that colonies of C. neoformans and related fungi growing on the ruins of the melted down reactor of the Chernobyl nuclear power plant may be able to use the energy of radiation for "radiotrophic" growth.[11]
Pathology
Infection with C. neoformans is termed cryptococcosis. Most infections with C. neoformans occur in the lungs.[12] However, fungal meningitis and encephalitis, especially as a secondary infection for AIDS patients, are often caused by C. neoformans, making it a particularly dangerous fungus. Infections with this fungus are rare in those with fully functioning immune systems.[13] So, C. neoformans is sometimes referred to as an opportunistic fungus.[13] It is a facultative intracellular pathogen[14] that can utilize host phagocytes to spread within the body.[15][16] Cryptococcus neoformans was the first intracellular pathogen for which the non-lytic escape process termed vomocytosis was observed.[17][18] It has been speculated that this ability to manipulate host cells results from environmental selective pressure by amoebae, a hypothesis first proposed by Arturo Casadevall under the term "accidental virulence".[19]
In human infection, C. neoformans is spread by inhalation of aerosolized basidiospores, and can disseminate to the central nervous system, where it can cause meningoencephalitis.[20] In the lungs, C. neoformans cells are phagocytosed by alveolar macrophages.[21] Macrophages produce oxidative and nitrosative agents, creating a hostile environment, to kill invading pathogens.[22] However, some C. neoformans cells can survive intracellularly in macrophages.[21] Intracellular survival appears to be the basis for latency, disseminated disease, and resistance to eradication by antifungal agents. One mechanism by which C. neoformans survives the hostile intracellular environment of the macrophage involves upregulation of expression of genes involved in responses to oxidative stress.[21]
Traversal of the blood–brain barrier by C. neoformans plays a key role in meningitis pathogenesis.[23] However, precise mechanisms by which it passes the blood-brain barrier are still unknown; one recent study in rats suggested an important role of secreted serine proteases.[24] The metalloprotease Mpr1 has been demonstrated to be critical in blood-brain barrier penetration.[25]
Meiosis (sexual reproduction), another possible survival factor for intracellular C. neoformans
The vast majority of environmental and clinical isolates of C. neoformans are mating type alpha. Filaments of mating type alpha have haploid nuclei ordinarily, but these can undergo a process of diploidization (perhaps by endoduplication or stimulated nuclear fusion) to form diploid cells termed blastospores. The diploid nuclei of blastospores are able to undergo meiosis, including recombination, to form haploid basidiospores that can then be dispersed.[26] This process is referred to as monokaryotic fruiting. Required for this process is a gene designated dmc1, a conserved homologue of genes recA in bacteria, and rad51 in eukaryotes (see articles recA and rad51). Dmc1 mediates homologous chromosome pairing during meiosis and repair of double-strand breaks in DNA.[27] One benefit of meiosis in C. neoformans could be to promote DNA repair in the DNA-damaging environment caused by the oxidative and nitrosative agents produced in macrophages.[26] Thus, C. neoformans can undergo a meiotic process, monokaryotic fruiting, that may promote recombinational repair in the oxidative, DNA-damaging environment of the host macrophage, and this may contribute to its virulence.
Serious complications
Infection starts in lungs, disseminates via blood to meninges and then to other parts of the body. Capsule inhibits phagocytosis. Can cause a systemic infection, including fatal meningitis known as meningoencephalitis in normal, diabetic and immunocompromised hosts. The infection from C. neoformans in the brain can be fatal if untreated. CNS (central nervous system) infection may also be present as a brain abscess known as cryptococcomas, subdural effusion, dementia, isolated cranial nerve lesion, spinal cord lesion, and ischemic stroke. If cryptococcal meningitis occurs, mortality rate is between 10–30%.[28]
Treatment
Cryptococcosis that does not affect the central nervous system can be treated with fluconazole alone.
Cryptococcal meningitis should be treated for two weeks with intravenous amphotericin B 0.7–1.0 mg/kg/day and oral flucytosine 100 mg/kg/day (or intravenous flucytosine 75 mg/kg/day if the patient is unable to swallow). This should then be followed by oral fluconazole 400–800 mg daily for ten weeks[29] and then 200 mg daily for at least one year and until the patient's CD4 count is above 200 cells/mcl.[30][31] Flucytosine is a generic, off-patent medicine. However, a market failure exists, with a two-week cost of flucytosine therapy being about $10,000. As a result, flucytosine is currently universally unavailable in low- and middle-income countries. In 1970, flucytosine was available in Africa.[32]
Intravenous ambisome 4 (mg/kg)/day may be used but is not superior; its main use is in patients who do not tolerate amphotericin B. The dose of 200 mg/kg/day for flucytosine is not more effective, is associated with more side effects and should not be used.
In Africa, oral fluconazole at a rate of 200 mg daily is often used. However, this does not result in cure, because it merely suppresses the fungus and does not kill it; viable fungus can continue to be grown from cerebrospinal fluid of patients not having taken fluconazole for many months. An increased dose of 400 mg daily does not improve outcomes,[33] but prospective studies from Uganda and Malawi reported that higher doses of 1200 mg per day have more fungicidal activity.[34] The outcomes with fluconazole monotherapy have 30% worse survival than amphotericin-based therapies, in a recent systematic review.[35]
References
- Buchanan, Kent; Murphy, J. W. (1998). "What Makes Cryptococcus neoformans a Pathogen? - Volume 4, Number 1—March 1998 - Emerging Infectious Disease journal - CDC". Emerging Infectious Diseases. 4 (1): 71–83. doi:10.3201/eid0401.980109. PMC 2627665. PMID 9452400.
- Ingavale, Susham S.; Chang, Yun C.; Lee, Hyeseung; McClelland, Carol M.; Leong, Madeline L.; Kwon-Chung, Kyung J. (2008-09-01). "Importance of Mitochondria in Survival of Cryptococcus neoformans Under Low Oxygen Conditions and Tolerance to Cobalt Chloride". PLoS Pathogens. 4 (9): e1000155. doi:10.1371/journal.ppat.1000155. ISSN 1553-7366. PMC 2528940. PMID 18802457.
- "What Makes Cryptococcus neoformans a Pathogen? - Volume 4, Number 1—March 1998 - Emerging Infectious Diseases - CDC". wwwnc.cdc.gov. Retrieved 2017-04-18
- Hagen, Ferry; Khayhan, Kantarawee; Theelen, Bart; Kolecka, Anna; Polacheck, Itzhack; Sionov, Edward; Falk, Rama; Parnmen, Sittiporn; Lumbsch, H. Thorsten (2015-05-01). "Recognition of seven species in the Cryptococcus gattii/Cryptococcus neoformans species complex". Fungal Genetics and Biology. 78: 16–48. doi:10.1016/j.fgb.2015.02.009. ISSN 1096-0937. PMID 25721988.
- "Archived copy". Archived from the original on 2012-04-01. Retrieved 2011-09-08.CS1 maint: archived copy as title (link)
- Bottone, E J (1980). "Cryptococcus neoformans: pitfalls in diagnosis through evaluation of gram-stained smears of purulent exudates". Journal of Clinical Microbiology. 12 (6): 790–1. PMC 273699. PMID 6171578.
- Zerpa, R; Huicho, L; Guillén, A (September 1996). "Modified India ink preparation for Cryptococcus neoformans in cerebrospinal fluid specimens" (PDF). Journal of Clinical Microbiology. 34 (9): 2290–1. PMC 229234. PMID 8862601.
- Shashikala; Kanungo, R; Srinivasan, S; Mathew, R; Kannan, M (Jul–Sep 2004). "Unusual morphological forms of Cryptococcus neoformans in cerebrospinal fluid". Indian Journal of Medical Microbiology. 22 (3): 188–90. PMID 17642731.
- Antinori, Spinello; Radice, Anna; Galimberti, Laura; Magni, Carlo; Fasan, Marco; Parravicini, Carlo (November 2005). "The role of cryptococcal antigen assay in diagnosis and monitoring of cryptococcal meningitis" (PDF). Journal of Clinical Microbiology. 43 (11): 5828–9. doi:10.1128/JCM.43.11.5828-5829.2005. PMC 1287839. PMID 16272534.
- Loftus BJ; et al. (2005). "The genome of the basidiomycetous yeast and human pathogen Cryptococcus neoformans". Science. 307 (5713): 1321–24. Bibcode:2005Sci...307.1321L. CiteSeerX 10.1.1.592.3649. doi:10.1126/science.1103773. PMC 3520129. PMID 15653466.
- Dadachova E; et al. (2007). Rutherford, Julian (ed.). "Ionizing Radiation Changes the Electronic Properties of Melanin and Enhances the Growth of Melanized Fungi". PLoS ONE. 2 (5): e457. Bibcode:2007PLoSO...2..457D. doi:10.1371/journal.pone.0000457. PMC 1866175. PMID 17520016.
- Tripathi, K; Mor, V; Bairwa, NK; Del Poeta, M; Mohanty, BK (2012). "Hydroxyurea treatment inhibits proliferation of Cryptococcus neoformans in mice". Front Microbiol. 3: 187. doi:10.3389/fmicb.2012.00187. PMC 3390589. PMID 22783238.
- What Makes Cryptococcus neoformans a Pathogen?, Kent L. Buchanan and Juneann W. Murphy University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma, USA
- Alvarez, M.; Burns, T.; Luo, Y.; Pirofski, L. A.; Casadevall, A. (2009). "The outcome of Cryptococcus neoformans intracellular pathogenesis in human monocytes". BMC Microbiology. 9: 51. doi:10.1186/1471-2180-9-51. PMC 2670303. PMID 19265539.
- Charlier, C; Nielsen, K; Daou, S; Brigitte, M; Chretien, F; Dromer, F (January 2009). "Evidence of a role for monocytes in dissemination and brain invasion by Cryptococcus neoformans". Infection and Immunity. 77 (1): 120–7. CiteSeerX 10.1.1.336.3329. doi:10.1128/iai.01065-08. PMC 2612285. PMID 18936186.
- Sabiiti, W; Robertson, E; Beale, MA; Johnston, SA; Brouwer, AE; Loyse, A; Jarvis, JN; Gilbert, AS; Fisher, MC; Harrison, TS; May, RC; Bicanic, T (May 2014). "Efficient phagocytosis and laccase activity affect the outcome of HIV-associated cryptococcosis". The Journal of Clinical Investigation. 124 (5): 2000–8. doi:10.1172/jci72950. PMC 4001551. PMID 24743149.
- Alvarez, M; Casadevall, A (7 November 2006). "Phagosome extrusion and host-cell survival after Cryptococcus neoformans phagocytosis by macrophages". Current Biology. 16 (21): 2161–5. Bibcode:1996CBio....6.1213A. doi:10.1016/j.cub.2006.09.061. PMID 17084702.
- Ma, H; Croudace, JE; Lammas, DA; May, RC (7 November 2006). "Expulsion of live pathogenic yeast by macrophages". Current Biology. 16 (21): 2156–60. Bibcode:1996CBio....6.1213A. doi:10.1016/j.cub.2006.09.032. PMID 17084701.
- Casadevall, A (2012). "Amoeba provide insight into the origin of virulence in pathogenic fungi". Recent Advances on Model Hosts. Advances in Experimental Medicine and Biology. 710. pp. 1–10. doi:10.1007/978-1-4419-5638-5_1. ISBN 978-1-4419-5637-8. PMID 22127880.
- Velagapudi R, Hsueh YP, Geunes-Boyer S, Wright JR, Heitman J (2009). "Spores as infectious propagules of Cryptococcus neoformans". Infect Immun. 77 (10): 4345–55. doi:10.1128/IAI.00542-09. PMC 2747963. PMID 19620339.
- Fan W, Kraus PR, Boily MJ, Heitman J (2005). "Cryptococcus neoformans gene expression during murine macrophage infection". Eukaryot Cell. 4 (8): 1420–1433. CiteSeerX 10.1.1.333.7376. doi:10.1128/EC.4.8.1420-1433.2005. PMC 1214536. PMID 16087747.
- Alspaugh JA, Granger DL (1991). "Inhibition of Cryptococcus neoformans replication by nitrogen oxides supports the role of these molecules as effectors of macrophage-mediated cytostasis". Infect Immun. 59 (7): 2291–2296. PMC 258009. PMID 2050398.
- Liu TB (2012). "Molecular mechanisms of cryptococcal meningitis". Virulence. 3 (2): 173–81. doi:10.4161/viru.18685. PMC 3396696. PMID 22460646.
- Xu CY (Feb 2014). "permeability of blood-brain barrier is mediated by serine protease during Cryptococcus meningitis". J Int Med Res. 42 (1): 85–92. doi:10.1177/0300060513504365. PMID 24398759.
- "Fungal protein found to cross blood-brain barrier".
- Lin X, Hull CM, Heitman J (2005). "Sexual reproduction between partners of the same mating type in Cryptococcus neoformans". Nature. 434 (7036): 1017–1021. Bibcode:2005Natur.434.1017L. doi:10.1038/nature03448. PMID 15846346.
- Michod RE, Bernstein H, Nedelcu AM (May 2008). "Adaptive value of sex in microbial pathogens". Infect Genet Evol. 8 (3): 267–285. doi:10.1016/j.meegid.2008.01.002. PMID 18295550.
- Public Health Agency of Canada
- Saag MS, Graybill RJ, Larsen RA, et al. (2000). "Practice guidelines for the management of cryptococcal disease. Infectious Diseases Society of America". Clin Infect Dis. 30 (4): 710–8. doi:10.1086/313757. PMID 10770733.
- Martínez E, García-Viejo MA, Marcos MA, et al. (2000). "Discontinuation of secondary prophylaxis for cryptococcal meningitis in HIV-infected patients responding to highly active antiretroviral therapy". AIDS. 14 (16): 2615–26. doi:10.1097/00002030-200011100-00029. PMID 11101078.
- Vibhagool A, Sungkanuparph S, Mootsikapun P, et al. (2003). "Discontinuation of secondary prophylaxis for Cryptococcal meningitis in Human Immunodeficiency Virus-infected patients treated with highly active antiretroviral therapy: a prospective, multicenter, randomized study". Clin Infect Dis. 36 (10): 1329–31. doi:10.1086/374849. PMID 12746781.
- Mpairwe Y, Patel KM (1970). "Cryptococcal meningitis in Mulago Hospital, Kampala". East Afr Med J. 47 (8): 445–7. PMID 5479794.
- CF Schaars; Meintjes GA; Morroni C; et al. (2006). "Outcome of AIDS-associated cryptococcal meningitis initially treated with 200 mg/day or 400 mg/day of fluconazole". BMC Infect Dis. 6: 118. doi:10.1186/1471-2334-6-118. hdl:11427/14193. PMC 1540428. PMID 16846523.
- Longley N, Muzoora C, Taseera K, Mwesigye J, Rwebembera J, Chakera A, Wall E, Andia I, Jaffar S, Harrison TS (2008). "Dose response effect of high-dose fluconazole for HIV-associated cryptococcal meningitis in southwestern Uganda". Clin Infect Dis. 47 (12): 1556–61. doi:10.1086/593194. PMID 18990067.
- Rajasingham R, Rolfes MA, Birkenkamp KE, Meya DB, Boulware DR (2012). "Cryptococcal meningitis treatment strategies in resource-limited settings: a cost-effectiveness analysis". PLoS Med. 9 (9): e1001316. doi:10.1371/journal.pmed.1001316. PMC 3463510. PMID 23055838.
External links
| Wikimedia Commons has media related to Cryptococcus neoformans. |