Crouzon syndrome
Crouzon syndrome is an autosomal dominant genetic disorder known as a branchial arch syndrome. Specifically, this syndrome affects the first branchial (or pharyngeal) arch, which is the precursor of the maxilla and mandible. Since the branchial arches are important developmental features in a growing embryo, disturbances in their development create lasting and widespread effects.
| Crouzon syndrome | |
|---|---|
 | |
| Baby with Crouzon syndrome | |
| Specialty | Medical genetics |
This syndrome is named after Octave Crouzon,[1][2] a French physician who first described this disorder. First called "craniofacial dysostosis" ("craniofacial" refers to the skull and face, and "dysostosis" refers to malformation of bone), the disorder was characterized by a number of clinical features which can be described by the rudimentary meanings of its former name. This syndrome is caused by a mutation in the fibroblast growth factor receptor 2 (FGFR2), located on chromosome 10. The developing fetus's skull and facial bones fuse early or are unable to expand. Thus, normal bone growth cannot occur. Fusion of different sutures leads to abnormal patterns of growth of the skull.
Signs and symptoms
.jpg)
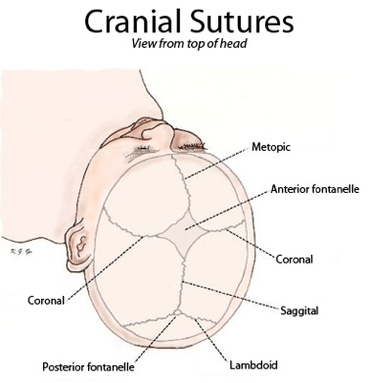
A defining characteristic of Crouzon syndrome is craniosynostosis, which results in an abnormal head shape. This is present in combinations of: turricephaly, frontal bossing, trigonocephaly (fusion of the metopic suture), brachycephaly (fusion of the coronal suture), dolichocephaly (fusion of the sagittal suture), plagiocephaly (unilateral premature closure of lambdoid and coronal sutures), oxycephaly (fusion of coronal and lambdoidal sutures), and complex craniosynostosis (premature closure of some or all sutures).
Exophthalmos (bulging eyes due to shallow eye sockets after early fusion of surrounding bones), hypertelorism (greater than normal distance between the eyes), and psittichorhina (beak-like nose) are also very common features. Other facial characteristics that are present in many cases include external strabismus and hypoplastic maxilla (insufficient growth of the midface), which results in relative mandibular prognathism (protruding chin) and gives the effect of the patient having a concave face.[3]
Most symptoms are secondary to the abnormal skull structure. Approximately 30% of people with Crouzon syndrome develop hydrocephalus. Sensorineural hearing loss is present in some cases. The abnormalities in the manner in which the eyes fit in the eye sockets can cause vision problems. Some people with the condition have a restricted airway and can experience severe problems breathing.[4]
Common features are a narrow/high-arched palate, posterior bilateral crossbite, hypodontia (missing some teeth), and crowding of teeth. Due to maxillary hypoplasia, people with Crouzon syndrome generally have a considerable permanent underbite.[5]
Causes
The current research indicates fibroblast growth factor receptors (FGFR) FGFR2 and FGFR3 as the leading factors in causing the autosomal dominant Crouzon syndrome.[6][7] These two transmembrane proteins are two of four fibroblast growth factor receptors involved in osteoblast differentiation during embryonic development; mutations amongst these receptors are involved in several genetic disorders.[6] There are 40 known mutations, most of which are caused by a missense mutation.[8] FGFR2 is the most commonly mutated gene, a missense at cysteine 342 in exon 9, which creates a gain-of-function.[8] The FGFR2lllc isoform, created via alternative splicing of exon 3 of the FGFR2 gene, uses exon 9 and is used in mesenchymal stem cells to control ossification. However, the mutation constitutively activates the transmembrane protein via a disulfide bond formed incorrectly due to the loss of cysteine 342.[8] FGFR3 is expressed more in the frontal bones during embryonic development, guiding cranial bone development. A point mutation causes constitutive activation of tyrosine in the activation loop, located in the cytosolic region of the protein, leading to accelerated differentiation of frontal osteoblasts,[9] resulting in premature fusion of frontal cranial bones.[9]
Diagnosis
Diagnosis of Crouzon syndrome usually can occur at birth by assessing the physical appearance of the infant. Further analysis, including radiographs, magnetic resonance imaging (MRI) scans, genetic testing, X-rays and CT scans can be used to confirm the diagnosis of Crouzon syndrome.
Treatment
Surgery is typically used to prevent the closure of sutures of the skull from damaging the brain's development. Without surgery, blindness and intellectual disability are typical outcomes. To move the orbits forward, surgeons expose the skull and orbits and reshape the bone. To treat the midface deficiency, surgeons can move the lower orbit and midface bones forward.
People with Crouzon syndrome tend to have multiple sutures involved, most specifically bilateral coronal craniosynostoses, and either open vault surgery or strip craniectomy (if child is under 6 months) can be performed. In the later scenario, a helmet is worn for several months following surgery.
Once treated for the cranial vault abnormalities, Crouzon patients generally go on to live a normal lifespan.
Epidemiology
Incidence of Crouzon syndrome is currently estimated to occur in 1.6 out of every 100,000 people[10] and is the most common craniostenosis syndrome.[7]
History
Crouzon syndrome was first described by Octave Crouzon in 1912.[11] He noted the affected patients were a mother and her daughter, implying a genetic basis.
References
- synd/1383 at Who Named It?
- L. E. O. Crouzon. Dysostose cranio-faciale héréditaire. Bulletin de la Société des Médecins des Hôpitaux de Paris, 1912, 33: 545-555.
- "Crouzon syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Retrieved 21 November 2018.
- "Crouzon Syndrome - NORD (National Organization for Rare Disorders)". NORD (National Organization for Rare Disorders). Retrieved 21 November 2018.
- Flint, Paul (2015). Cummings Otolaryngology (6 ed.). Elsevier. pp. 2891–2914.
- Snyder-Warwick AK, Perlyn CA, Pan J, Yu K, Zhang L, Ornitz DM (February 2010). "Analysis of a gain-of-function FGFR2 Crouzon mutation provides evidence of loss of function activity in the etiology of cleft palate". Proc. Natl. Acad. Sci. U.S.A. 107 (6): 2515–20. Bibcode:2010PNAS..107.2515S. doi:10.1073/pnas.0913985107. PMC 2823872. PMID 20133659.
- Reference, Genetics Home. "Crouzon syndrome". Genetics Home Reference. Retrieved 21 November 2018.
- Fenwick AL, Goos JA, Rankin J, Lord H, Lester T, Hoogeboom AJ, van den Ouweland AM, Wall SA, Mathijssen IM, Wilkie AO (August 2014). "Apparently synonymous substitutions in FGFR2 affect splicing and result in mild Crouzon syndrome". BMC Med. Genet. 15: 95. doi:10.1186/s12881-014-0095-4. PMC 4236556. PMID 25174698.
- Di Rocco F, Biosse Duplan M, Heuzé Y, Kaci N, Komla-Ebri D, Munnich A, Mugniery E, Benoist-Lasselin C, Legeai-Mallet L (June 2014). "FGFR3 mutation causes abnormal membranous ossification in achondroplasia". Hum. Mol. Genet. 23 (11): 2914–25. doi:10.1093/hmg/ddu004. PMID 24419316.
- Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LH, Stephens K, Amemiya A, Robin NH, Falk MJ, Haldeman-Englert CR (October 20, 1998). "FGFR-Related Craniosynostosis Syndromes". GeneReviews. PMID 20301628.
- Rodriguez, Eduardo (2018). Plastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic Surgery (4 ed.). Elsevier.
External links
| Classification | |
|---|---|
| External resources |
| Wikimedia Commons has media related to Crouzon syndrome. |
- Crouzon syndrome on Genetics Home Reference from U.S. National Library of Medicine & National Institutes of Health
- GeneReviews/NIH/NCBI/UW entry on FGFR-Related Craniosynostosis Syndromes