Conduction aphasia
Conduction aphasia, also called associative aphasia, is a relatively rare form of aphasia. An acquired language disorder, it is characterized by intact auditory comprehension, fluent (yet paraphasic) speech production, but poor speech repetition. They are fully capable of understanding what they are hearing, but fail to encode phonological information for production. This deficit is load-sensitive as patients show significant difficulty repeating phrases, particularly as the phrases increase in length and complexity and as they stumble over words they are attempting to pronounce.[1][2] Patients will display frequent errors during spontaneous speech, such as substituting or transposing sounds. They will also be aware of their errors, and will show significant difficulty correcting them.[3] For example: "Clinician: Now, I want you to say some words after me. Say ‘boy’. Patient: Boy. Clinician: Home. Patient: Home. Clinician: Seventy-nine. Patient: Ninety-seven. No … sevinty-sine … siventy-nice…. Clinician: Let’s try another one. Say ‘refrigerator’. Patient: Frigilator … no? how about … frerigilator … no frigaliterlater … aahh! It’s all mixed up!" [4]
| Conduction aphasia | |
|---|---|
| Other names | Associative aphasia |
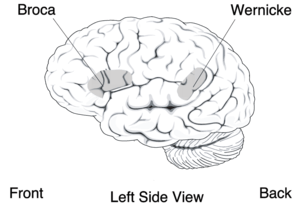 | |
| Broca's area and Wernicke's area | |
| Specialty | Neurology |
Shallice and Warrington (1970) were able to differentiate two variants of this constellation: the reproduction and the repetition type. These authors suggested an exclusive deficit of auditory-verbal short-term memory in repetition conduction aphasia whereas the other variant was assumed to reflect disrupted phonological encoding mechanism, afflicting confrontation tasks such as repetition, reading and naming in a similar manner.[5]
Left-hemisphere damage involving auditory regions often result in speech deficits. Lesions in this area that damage the sensorimotor dorsal stream suggest that the sensory system aid in motor speech. Studies have suggested that conduction aphasia is a result of damage specifically to the left superior temporal gyrus and/or the left supra marginal gyrus.[6] The classical explanation for conduction aphasia is that of a disconnection between the brain areas responsible for speech comprehension (Wernicke's area) and speech production (Broca's area), due specifically to damage to the arcuate fasciculus, a deep white matter tract. Patients are still able to comprehend speech because the lesion does not disrupt the ventral stream pathway.
Signs and symptoms
Conduction aphasics will show relatively well-preserved auditory comprehension, which may even be completely functional. All cases are individualized and unique to their own extent. Spontaneous speech production will be fluent and generally grammatically and syntactically correct. Intonation and articulation will also be preserved. Speech will often contain paraphasic errors: phonemes and syllables will be dropped or transposed (e.g., "snowball" → "snowall", "television" → "vellitision", "ninety-five percent" → "ninety-twenty percent"). The hallmark deficit of this disorder, however, is in repetition. Patients will show a marked inability to repeat words or sentences when prompted by an examiner.[7][8] After saying a sentence to a person with conduction aphasia, he or she will be able to paraphrase the sentence accurately but will not be able to repeat it. This is possibly because their "motor speech error processing is disrupted by inaccurate forward predictions, or because detected errors are not translated into corrective commands due to damage to the auditory-motor interface".[9][10] When prompted to repeat words, patients will be unable to do so, and produce many paraphasic errors. For example, when prompted with "bagger", a patient may respond with, "gabber".[11] Recent summaries (Brown, 1972; Benson, Sheremata, Bouchard, Segarra, Price, & Geschwind, 1973) that describe the syndrome of conduction aphasia emphasize a contrast between the defective speech and writing of patients and their relatively good comprehension. The spontaneous speech of a conduction aphasic is fluent, yet it is circumlocutory and inadequately structured. Patients have difficulty in finding words appropriate to a context and in pronouncing words accurately. Failures in naming, reading aloud, and repeating are quite evident. Performances in naming tasks typically demonstrate an impaired ability to find words for presented objects, for body parts, and for colors. Oral reading is likely to be laborious and attended by the same errors that occur in spontaneous speech [12]
However, patients recognize their paraphasias and errors and will try to correct them. Typically, a patient will make multiple attempts correcting phonological speech errors until they are successful. This recognition is due to preserved auditory error detection mechanisms.[10] Error sequences frequently fit a pattern of incorrect approximations. These common errors typically occur in morphemes that a) share one or more similarly located phonemes but b) differ in at least one aspect that makes the substituted morpheme(s) semantically distinct. This repetitive effort to approximate the appropriate word or phrase is known as conduite d’approche.[8] Repetitive self correction is commonly used by patients of conduction aphasia. Due to their relatively preserved auditory comprehension, conduction aphasics are capable of accurately monitoring, and attempting to correct, their own errors in speech output. [13]For example, when prompted to repeat "Rosenkranz", a German-speaking patient may respond with, "rosenbrau... rosenbrauch... rosengrau... bro... grosenbrau... grossenlau, rosenkranz,... kranz... rosenkranz".[11]
Conduction aphasia is a relatively mild language impairment, and most patients return to day-to-day life.[11][14] Broca's and Wernicke's aphasia are relatively common in middle cerebral artery strokes. Pure conduction aphasia which affects only repetition not common. [15]Symptoms of conduction aphasia, as with other aphasias, can be transient, sometimes lasting only several hours or a few days. As aphasias and other language disorders are frequently due to stroke, their symptoms can change and evolve over time, or simply disappear. If the cause is a stroke, patients can make a good recovery but may have persistent deficits. [16] This is because the healing in the brain after inflammation or hemorrhage, leads to decreased local impairment. Furthermore, the plasticity of the brain may allow the recruitment of new pathways to restore lost function. For example, the right hemisphere speech systems may learn to correct for left-hemisphere damage. However, chronic conduction aphasia is possible, without transformation to other aphasias.[11] These patients show prolonged, profound deficits in repetition, frequent phonemic paraphasias, and conduite d'approche during spontaneous speech.
Causes
Conduction aphasia is caused by damage to the parietal lobe of the brain, especially in regards to the area associated with the left-hemisphere dominant dorsal stream network.[17][10] The arcuate fasciculus, which connects Broca's area and Wernicke's area (important for speech and language production and comprehension, respectively), is affected.[17] These two areas control speech and language in the brain. The arcuate fasciculus is a thick band of fiber that connects the two areas and carries messages between them. When this area is damaged, the patient experiences damage to the auditory-motor integration system. This results in disruption to the delayed auditory feedback network, causing the individual to have difficulty correcting themselves on speech repetition tasks.[10] Additionally, recent evidence suggests that conduction aphasia can also be caused by lesions in the left superior temporal gyrus and/or the left supramarginal gyrus.[6]
The brain damage causing conduction aphasia is often from a stroke, which can produce both localized and widespread damage. Traumatic brain injury and tumors can also lead to localized lesions, with potential to cause conduction aphasia. Conduction aphasia can also be seen in cases of cortical damage without subcortical extensions.[18]
Pathophysiology
Traditionally, it has been believed that conduction aphasia was the result of a lesion in the arcuate fasciculus, a deep, white matter bundle connecting the posterior temporoparietal junction with the frontal cortex. It was thought that this bundle transmitted information between Wernicke's area (responsible for language comprehension) and Broca's area (responsible for language production). Wernicke, and later Lichtheim and others, theorized that a disconnect between these two regions caused patients to fail to monitor speech and limited their ability to transfer information between comprehension and production functions, thus leading to paraphasic errors and a deficit in repetition of auditory input. This hypothesis fits well with the Wernicke-Geschwind model of language, which compartmentalizes and localizes speech comprehension and production.
Recent research has pointed to a different explanation for conduction aphasia, similar to Wernicke's, which is based on newer models suggesting language is facilitated by "cortically based, anatomically distributed, modular networks."[19] Anderson et al. describe an experiment in which electrical stimulation of the left posterior superior temporal cortex in a human subject induced symptoms consistent with conduction aphasia, indicating that a deep brain disconnection is not necessary.[19] While this study does not completely discredit the disconnection hypothesis, it points to a system in which transmission of spoken language information involves more than just the arcuate fasciculus. Regardless of the role that the arcuate fasciculus plays in the disorder, the cortical component evidently plays a role as well.
Diagnosis
Individuals with conduction aphasia are able to express themselves fairly well, with some word finding and functional comprehension difficulty.[20] Although people with aphasia may be able to express themselves fairly well, they tend to have issues repeating phrases, especially phrases that are long and complex.[20] During the assessment of aphasia, the clinician should examine the patient's verbal fluency, comprehension, repetition, reading, writing, and naming. When asked to repeat something, the patient will be unable to do so without significant difficulty, repeatedly attempting to self-correct (conduite d'approche).
Several standardized test batteries exist for diagnosing and classifying aphasias. These tests are capable of identifying conduction aphasia with relative accuracy.[8] The Boston Diagnostic Aphasia Examination (BDAE) and the Western Aphasia Battery (WAB) are two commonly used test batteries for diagnosing conduction aphasia. These examinations involve a set of tests, which include asking patients to name pictures, read printed words, count aloud, and repeat words and non-words (such as shwazel). Neuro-imaging should also be used to look for a stroke, tumor, infection, or another pathology in the setting of conduction aphasia. This can be done through a CT or MRI or the brain; these are the first imaging modality of choice.[21]
Treatment
There is not standard treatment for aphasia; speech and language therapy are typically used. There are no medical or surgical treatments. Treatment for aphasias is generally individualized, focusing on specific language and communication improvements, and regular exercise with communication tasks. Regular therapy for conduction aphasics has been shown to result in steady improvement on the Western Aphasia Battery.[22] The Western Aphasia Battery assesses neurological disorders to discern the degree and type of aphasia present. The test also discerns a patient’s strengths and weaknesses, which can be used to treat the patient better. Therapists should tailor treatment to the individual needs of the patient. The main focus for during speech therapy for conduction aphasia patients is to strengthen correct word usage and auditory comprehension. A major goal is to focus on repetition.
History
In the late 19th century, Paul Broca studied patients with expressive aphasia. These patients had lesions in the anterior perisylvian region (now known as Broca's area), and produced halting and labored speech, lacking in function words and grammar. For example, "clinician: What brought you to the hospital? patient: yes … ah … Monday … ah … Dad … Peter Hogan, and Dad … ah … hospital … and ah … Wednesday … Wednesday … nine o’clock and ah Thursday … ten o’clock … doctors two … two … an doctors and … ah … teeth … yah … and a doctor an girl … and gums, an I." [23] Comprehension is generally preserved, although there can be deficits in interpretation of complex sentences. In an extreme example, one of his patients could only produce a single syllable, "Tan".
Meanwhile, Carl Wernicke described patients with receptive aphasia, who had damage to the left posterior superior temporal lobe, which he named "the area of word images". These patients could speak fluently, but their speech lacked meaning. They had a severe deficit in auditory comprehension. For example, "Clinician: What brings you to the hospital? Patient: Boy, I’m sweating, I’m awful nervous, you know, once in a while I get caught up, I can’t mention the tarripote, a month ago, quite a little, I’ve done a lot well, I impose a lot, while on the other hand, you know what I mean, I have to run around, look it over, trebbin and all that sort of stuff."[24]
The two disorders (expressive and receptive aphasias) thus seemed complementary, and corresponded to two distinct anatomical locations.
Wernicke predicted the existence of conduction aphasia in his landmark 1874 monograph, Der Aphasische Symptomenkompleks: Eine Psychologische Studie auf Anatomischer Basis.[3][19][25] He was the first to distinguish the various aphasias in an anatomical framework, and proposed that a disconnection between the two speech systems (motor and sensory) would lead to a unique condition, distinct from both expressive and receptive aphasias, which he termed Leitungsaphasie. He did not explicitly predict the repetition deficit, but did note that, unlike those with Wernicke's aphasia, conduction aphasics would be able to comprehend speech properly, and intriguingly, would be able to hear and understand their own speech errors, leading to frustration and self-correction.[25][26]
Wernicke was influenced by Theodor Meynert, his mentor, who postulated that aphasias were due to perisylvian lesions. Meynert also distinguished between the posterior and anterior language systems, leading Wernicke to localize the two regions.[19] Wernicke's research into the fiber pathways connecting the posterior and anterior regions lead him to theorize that damage to the fibers under the insula would lead to conduction aphasia. Ludwig Lichtheim expanded on Wernicke's work, although he labeled the disorder commissural aphasia, to distinguish between aphasias tied to processing centers.[27]
Sigmund Freud would argue in 1891 that the old framework was inaccurate; the entire perisylvian area, from the posterior to the anterior regions, were equivalent in facilitating speech function. In 1948 Kurt Goldstein postulated that spoken language was a central phenomenon, as opposed to a differentiated and disparate set of functionally distinct modules. To Freud and Goldstein, conduction aphasia was thus the result of a central, core language breakdown; Goldstein labeled the disorder central aphasia.[19]
Later work and examination of brain structures, however, implicated the arcuate fasciculus, a white matter bundle connecting the posterior temporoparietal junction with the frontal cortex. Norman Geschwind proposed that damage to this bundle caused conduction aphasia; the characteristic deficits in auditory repetition were due to failed transmission of information between the two language centers.[19] Studies showed that conduction aphasics had an intact 'inner voice', which discredited the central deficit model of Freud and Goldstein.[28] The Wernicke-Lichtheim-Geschwind disconnection hypothesis thus became the prevailing explanation for conduction aphasia. However, recent reviews and research have cast doubt on the singular role of the arcuate fasciculus and the model of spoken language in general.
See also
|
|
|
References
- Conduction Aphasia. (n.d.). Retrieved from http://www.asha.org/Glossary/Conduction-Aphasia/
- Carlson, Neil R.; Heth, C. Donald (2007). Psychology the science of behaviour (4th ed.). Pearson Education Inc. ISBN 0-205-64524-0.
- Gazzaniga, Michael S.; Ivry, Richard B.; Mangun, George R. (2002). Cognitive neuroscience: the biology of the mind. New York: W. W. Norton. p. 389. ISBN 0-393-97777-3.
- Robert H. Brookshire. An Introduction to Neurogenic Communication Disorders, 6e. volume. Mosby Year Book, St. Louis, 2003.
- Sidiropoulos, Kyriakos; De Bleser, Ria; Ackermann, Hermann; Preilowski, Bruno (2008). "Pre-lexical disorders in repetition conduction aphasia". Neuropsychologia. 46 (14): 3225–38. doi:10.1016/j.neuropsychologia.2008.07.026. PMID 18761023.
- Tippett, Donna C; Hillis, Argye E (2016). "Vascular Aphasia Syndromes". In Hickok, Gregory; Small, Steven L. (eds.). Neurobiology of Language. pp. 913–22. doi:10.1016/B978-0-12-407794-2.00073-0. ISBN 978-0-12-407794-2.
- Damasio, Hanna; Damasio, Antonio R (1980). "The Anatomical Basis of Conduction Aphasia". Brain. 103 (2): 337–50. doi:10.1093/brain/103.2.337. PMID 7397481.
- Kohn, Susan E. (1992). Conduction aphasia. Hillsdale, N.J: L. Erlbaum. pp. 40–42. ISBN 0-8058-0681-4.
- Manasco, Hunter (2017). "The Aphasias". Introduction to Neurogenic Communication Disorders. pp. 93–44. ISBN 978-1-284-10072-3.
- Behroozmand, Roozbeh; Phillip, Lorelei; Johari, Karim; Bonilha, Leonardo; Rorden, Chris; Hickok, Gregory; Fridriksson, Julius (2018). "Sensorimotor impairment of speech auditory feedback processing in aphasia". NeuroImage. 165: 102–11. doi:10.1016/j.neuroimage.2017.10.014. PMC 5732035.
- Bartha, Lisa; Benke, Thomas (2003). "Acute conduction aphasia: An analysis of 20 cases". Brain and Language. 85 (1): 93–108. doi:10.1016/S0093-934X(02)00502-3. PMID 12681350.
- ""Conduction Aphasia." Conduction Aphasia - an Overview". ScienceDirect Topics.
- Buschbaum, Bradley R; et al. ""Conduction Aphasia, Sensory-Motor Integration, and Phonological Short-Term Memory - an Aggregate Analysis of Lesion and FMRI Data." Brain and Language". U.S. National Library of Medicine, Dec. 2011. Explicit use of et al. in:
|first1=(help) - Benson, D. Frank; Sheremata, W. A; Bouchard, R; Segarra, J. M; Price, D; Geschwind, N (1973). "Conduction Aphasia". Archives of Neurology. 28 (5): 339–46. doi:10.1001/archneur.1973.00490230075011. PMID 4696016.
- Acharya, Aninda B. ""Conduction Aphasia." StatPearls [Internet]". U.S. National Library of Medicine, 29 June 2019.
- Acharya, Aninda B. ""Conduction Aphasia." StatPearls [Internet]". U.S. National Library of Medicine, 29 June 2019.
- Manasco, M. Hunter (2014). Introduction to Neurogenic Communication Disorders. Jones & Bartlett Learning.
- Ardila, Alfredo (2010). "A Review of Conduction Aphasia". Current Neurology and Neuroscience Reports. 10 (6): 499–503. doi:10.1007/s11910-010-0142-2. PMID 20711691.
- Anderson, J.M; Gilmore, R; Roper, S; Crosson, B; Bauer, R.M; Nadeau, S; Beversdorf, D.Q; Cibula, J; Rogish, M; Kortencamp, S; Hughes, J.D; Gonzalez Rothi, L.J; Heilman, K.M (1999). "Conduction Aphasia and the Arcuate Fasciculus: A Reexamination of the Wernicke–Geschwind Model". Brain and Language. 70 (1): 1–12. doi:10.1006/brln.1999.2135. PMID 10534369.
- "Conduction Aphasia". www.asha.org. Retrieved 2015-11-13.
- Acharya, Aninda B. ""Conduction Aphasia." StatPearls [Internet]". U.S. National Library of Medicine, 29 June 2019.
- Bakheit, A.M.O; Shaw, S; Carrington, S; Griffiths, S (2016). "The rate and extent of improvement with therapy from the different types of aphasia in the first year after stroke". Clinical Rehabilitation. 21 (10): 941–9. doi:10.1177/0269215507078452. PMID 17981853.
- Howard, H. (2017, October 7). Cerebral cortex. Retrieved from http://www.tulane.edu/~howard/BrLg/Cortex.html
- Howard, H. (2017, October 7). Cerebral cortex. Retrieved from http://www.tulane.edu/~howard/BrLg/Cortex.html
- Kohn, Susan E. (1992). Conduction aphasia. Hillsdale, N.J: L. Erlbaum. pp. 25–26. ISBN 0-8058-0681-4.
- Köhler, Kerstin; Bartels, Claudius; Herrmann, Manfred; Dittmann, Jürgen; Wallesch, Claus-W (1998). "Conduction aphasia—11 classic cases". Aphasiology. 12 (10): 865–84. doi:10.1080/02687039808249456.
- Kohn, Susan E. (1992). Conduction aphasia. Hillsdale, N.J: L. Erlbaum. pp. 28–29. ISBN 0-8058-0681-4.
- Feinberg, T. E; Rothi, L. J. G; Heilman, K. M (1986). "'Inner Speech' in Conduction Aphasia". Archives of Neurology. 43 (6): 591–3. doi:10.1001/archneur.1986.00520060053017. PMID 3718287.
Further reading
- Hickok, Gregory; Buchsbaum, Bradley; Humphries, Colin; Muftuler, Tugan (2003). "Auditory–Motor Interaction Revealed by fMRI: Speech, Music, and Working Memory in Area Spt". Journal of Cognitive Neuroscience. 15 (5): 673–82. doi:10.1162/089892903322307393. PMID 12965041.
- Hickok, Gregory; Poeppel, David (2004). "Dorsal and ventral streams: A framework for understanding aspects of the functional anatomy of language". Cognition. 92 (1–2): 67–99. doi:10.1016/j.cognition.2003.10.011. PMID 15037127.
- Baldo, J; Klostermann, E; Dronkers, N (2008). "It's either a cook or a baker: Patients with conduction aphasia get the gist but lose the trace". Brain and Language. 105 (2): 134–40. doi:10.1016/j.bandl.2007.12.007. PMID 18243294.
- Carlson, Neil R.; Heth, C. Donald (2007). Psychology the science of behaviour (4th ed.). Pearson Education Inc. ISBN 0-205-64524-0.
- Sidiropoulos, Kyriakos; Ackermann, Hermann; Wannke, Michael; Hertrich, Ingo (2010). "Temporal processing capabilities in repetition conduction aphasia". Brain and Cognition. 73 (3): 194–202. doi:10.1016/j.bandc.2010.05.003. PMID 20621742.