Cimino fistula
A Cimino fistula, also Cimino-Brescia fistula, surgically created arteriovenous fistula and (less precisely) arteriovenous fistula (often abbreviated AV fistula or AVF), is a type of vascular access for hemodialysis. It is typically a surgically created connection between an artery and a vein in the arm, although there have been acquired arteriovenous fistulas which do not in fact demonstrate connection to an artery.[1]

Theoretical basis
Surgically created AV fistulas work effectively because they:
History
The procedure was invented by doctors James Cimino and M. J. Brescia in 1966.[3] Before the Cimino fistula was invented, access was through a Scribner shunt, which consisted of a Teflon tube with a needle at each end. Between treatments, the needles were left in place and the tube allowed blood flow to reduce clotting. But Scribner shunts lasted only a few days to weeks. Frustrated by this limitation, James E. Cimino recalled his days as a phlebotomist (blood drawer) at New York City's Bellevue Hospital in the 1950s when Korean War veterans showed up with fistulas caused by trauma. Cimino recognized that these fistulas did not cause the patients harm and were easy places to get repeated blood samples. He convinced surgeon Kenneth Appell to create some in patients with chronic kidney failure and the result was a complete success. Scribner shunts were quickly replaced with Cimino fistulas, and they remain the most effective, longest-lasting method for long-term access to patients' blood for hemodialysis today.
Anatomy
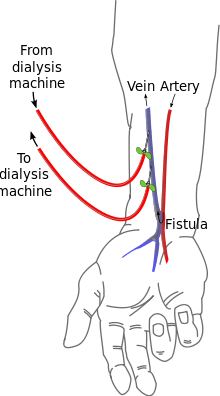
The radiocephalic arteriovenous fistula (RC-AVF) is a shortcut between cephalic vein and radial artery at the wrist. It is the recommended first choice for hemodialysis access. Possible underlying causes for failure are stenosis and thrombosis especially in diabetics and those with low blood flow such as due to narrow vessels, arteriosclerosis and advanced age. Reported patency of fistulae after 1 year is about 62.5%.[4]
See also
References
- "Case Report : Acquired Arteriovenous Fistula of the Right Forearm Caused by Repeated Blunt Trauma: a Report of a Rare Case" (PDF). Atcs.jp. Retrieved 2013-09-08.
- Konner K (2002). "Vascular access in the 21st century". J. Nephrol. 15 Suppl 6: S28–32. PMID 12515371.
- Brescia MJ, Cimino JE, Appel K, Hurwich BJ (1966). "Chronic hemodialysis using venipuncture and a surgically created arteriovenous fistula". N. Engl. J. Med. 275 (20): 1089–92. doi:10.1056/NEJM196611172752002. PMID 5923023.
- 1A. A. Al-Jaishi; M. J. Oliver; S. M. Thomas; C. E. Lok (2014). "Patency Rates of the Arteriovenous Fistula for Hemodialysis: A Systematic Review and Meta-analysis". Cite journal requires
|journal=(help)