Cherry angioma
Cherry angiomas, also known as Campbell De Morgan spots or senile angiomas,[1] are cherry red[2] papules on the skin. They are a harmless benign tumor, containing an abnormal proliferation of blood vessels, and have no relationship to cancer. They are the most common kind of angioma, and increase with age, occurring in nearly all adults over 30 years.
| Cherry angioma | |
|---|---|
 | |
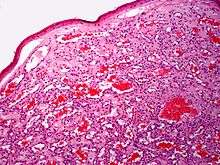
| A cherry angioma | |
| Specialty | Cardiology |
Campbell de Morgan is the nineteenth-century British surgeon who first described them.
Signs and symptoms
Cherry angiomas are made up of clusters of capillaries at the surface of the skin,[3] forming a small round dome ("papule"),[3] which may be flat topped . They range in colour from bright red to purple. When they first develop, they may be only a tenth of a millimeter in diameter and almost flat, appearing as small red dots. However, they then usually grow to about one or two millimeters across, and sometimes to a centimeter or more in diameter . As they grow larger, they tend to expand in thickness, and may take on the raised and rounded shape of a dome. Multiple adjoining angiomas form a polypoid angioma.[3] Because the blood vessels comprising an angioma are so close to the skin's surface, cherry angiomas may bleed profusely if they are injured.[3]
One study found that the majority of capillaries in cherry hemangiomas are fenestrated and stain for carbonic anhydrase activity.[4]
Cause
Cherry angiomas appear spontaneously in many people in middle age but can also, less commonly, occur in young people. They can also occur in an aggressive eruptive manner in any age. The underlying cause for the development of cherry angiomas is not understood.
Cherry angioma may occur through two different mechanisms: angiogenesis (the formation of new blood vessels from pre-existing vessels), and vasculogenesis (the formation of totally new vessels, which usually occurs during embryonic and fetal development).[5]
One study published in 2010 found that a regulatory nucleic acid suppresses protein growth factors that cause vascular growth. This regulatory nucleic acid was lower in tissue samples of hemangiomas, and the growth factors were elevated, which suggests that the elevated growth factors may cause hemangiomas.[6] The study found that the level of microRNA 424 is significantly reduced in senile hemangiomas compared to normal skin resulting in increased protein expression of MEK1 and cyclin E1. By inhibiting mir-424 in normal endothelial cells they could observe the same increased protein expression of MEK1 and cyclin E1 which, important for the development of senile hemangioma, induced cell proliferation of the endothelial cells. They also found that targeting MEK1 and cyclin E1 with small interfering RNA decreased the number of endothelial cells.
A study published in 2019 identified that somatic mutations in GNAQ and GNA11 genes[7] are present in many cherry angiomas. These specific missense mutations found in hemangiomas are also associated with port-wine stains and uveal melanoma.
Chemicals and compounds that have been seen to cause cherry angiomas are mustard gas,[8][9][10][11] 2-butoxyethanol,[12] bromides,[13] and cyclosporine.[14]
A significant increase in the density of mast cells has been seen in cherry hemangiomas compared with normal skin.[15]
Diagnosis
The diagnosis is based on the clinical appearance of the lesions. Examination with a dermatoscope shows characteristic red, purple, or blue-black lagoons.
Treatment
These lesions generally do not require treatment. If they are cosmetically unappealing or are subject to bleeding angiomas may be removed by electrocautery, a process of destroying the tissue by use of a small probe with an electric current running through it.[16] Removal may cause scarring. More recently pulsed dye laser or intense pulsed light (IPL) treatment has also been used.[17][18]
Future treatment based on a locally acting inhibitor of MEK1 and Cyclin E1 could possibly be an option. A natural MEK1 inhibitor is myricetin[19][20]
Prognosis
In most patients, the number and size of cherry angiomas increases with advancing age. They are harmless, having no relation to cancer at all.[21]
Epidemiology
Cherry angiomas occur in all races, ethnic backgrounds, and sexes.
References
- James, William; Berger, Timothy; Elston, Dirk (2006). Andrews' Diseases of the Skin: Clinical Dermatology (10th ed.). Philadelphia: Saunders. p. 595. ISBN 978-0-7216-2921-6. OCLC 62736861.
- "cherry angioma" at Dorland's Medical Dictionary
- Stockman, David L. (2016). Diagnostic pathology. Vascular. Philadelphia, PA: Elsevier. pp. 3.4–3.5. ISBN 978-0-323-37674-7.
- Eichhorn, M; Jungkunz, W; Wörl, J; Marsch, WC (1994). "Carbonic anhydrase is abundant in fenestrated capillaries of cherry hemangioma". Acta Dermato-venereologica. 74 (1): 51–3. doi:10.2340/00015555745153 (inactive 2019-08-20). PMID 7908484.
- Kishimoto, Saburo; Hideya Takenaka; Hideya Takenaka; Hideya Takenaka; Hirokazu Yasuno (2000). "Glomeruloid hemangioma in POEMS syndrome shows two different immunophenotypic endothelial cells". Cutaneous Pathology. 27 (2): 87–92. doi:10.1034/j.1600-0560.2000.027002087.x.
- Nakashima, T; Jinnin, M; Etoh, T; Fukushima, S; Masuguchi, S; Maruo, K; Inoue, Y; Ishihara, T; Ihn, H (2010). Egles, Christophe (ed.). "Down-regulation of mir-424 contributes to the abnormal angiogenesis via MEK1 and cyclin E1 in senile hemangioma: its implications to therapy". PLoS ONE. 5 (12): e14334. Bibcode:2010PLoSO...514334N. doi:10.1371/journal.pone.0014334. PMC 3001869. PMID 21179471.
- Klebanov, Nikolai; Lin, William M.; Artomov, Mykyta; Shaughnessy, Michael; Njauw, Ching-Ni; Bloom, Romi; Eterovic, Agda Karina; Chen, Ken; Kim, Tae-Beom (2019-01-02). "Use of Targeted Next-Generation Sequencing to Identify Activating Hot Spot Mutations in Cherry Angiomas". JAMA Dermatology. 155 (2): 211–215. doi:10.1001/jamadermatol.2018.4231. ISSN 2168-6084. PMC 6440195. PMID 30601876.
- Firooz, Alireza; Komeili, Ali; Dowlati, Yahya (1999). "Eruptive melanocytic nevi and cherry angiomas secondary to exposureto sulfur mustard gas". Journal of the American Academy of Dermatology. 40 (4): 646–7. doi:10.1016/S0190-9622(99)70460-3. PMID 10188695.
- Hefazi, Mehrdad; Maleki, Masoud; Mahmoudi, Mahmoud; Tabatabaee, Abbas; Balali-Mood, Mahdi (2006). "Delayed complications of sulfur mustard poisoning in the skin and the immune system of Iranian veterans 16–20 years after exposure". International Journal of Dermatology. 45 (9): 1025–31. doi:10.1111/j.1365-4632.2006.03020.x. PMID 16961503.
- Ma, Hui-Jun; Zhao, Guang; Shi, Fei; Wang, Yi-Xia (2006). "Eruptive cherry angiomas associated with vitiligo: Provoked by topical nitrogen mustard?". The Journal of Dermatology. 33 (12): 877–9. doi:10.1111/j.1346-8138.2006.00200.x. PMID 17169094.
- Emadi, Seyed Naser; Hosseini-Khalili, Alireza; Soroush, Mohammad Reza; Davoodi, Seyed Masoud; Aghamiri, Seyed Samad (2008). "Mustard gas scarring with specific pigmentary, trophic and vascular characteristics (case report, 16-year post-exposure)". Ecotoxicology and Environmental Safety. 69 (3): 574–6. doi:10.1016/j.ecoenv.2007.01.003. PMID 17382390.
- Raymond, Lawrence W.; Williford, Linda S.; Burke, William A. (1998). "Eruptive Cherry Angiomas and Irritant Symptoms After One Acute Exposure to the Glycol Ether Solvent 2-Butoxyethanol". Journal of Occupational & Environmental Medicine: 1059–64. doi:10.1097/00043764-199812000-00005.
- Cohen, Arnon D.; Cagnano, Emanuela; Vardy, Daniel A. (2001). "Cherry Angiomas Associated with Exposure to Bromides". Dermatology. 202 (1): 52–3. doi:10.1159/000051587. PMID 11244231.
- De Felipe, I.; Redondo, P (1998). "Eruptive Angiomas After Treatment With Cyclosporine in a Patient With Psoriasis". Archives of Dermatology. 134 (11): 1487–8. doi:10.1001/archderm.134.11.1487. PMID 9828895.
- Hagiwara, K; Khaskhely, NM; Uezato, H; Nonaka, S (1999). "Mast cell "densities" in vascular proliferations: a preliminary study of pyogenic granuloma, portwine stain, cavernous hemangioma, cherry angioma, Kaposi's sarcoma, and malignant hemangioendothelioma". The Journal of Dermatology. 26 (9): 577–86. doi:10.1111/j.1346-8138.1999.tb02052.x. PMID 10535252.
- Aversa, AJ; Miller Of, 3rd (1983). "Cryo-curettage of cherry angiomas". The Journal of Dermatologic Surgery and Oncology. 9 (11): 930–1. doi:10.1111/j.1524-4725.1983.tb01042.x. PMID 6630708.
- Dawn, G.; Gupta, G. (2003). "Comparison of potassium titanyl phosphate vascular laser and hyfrecator in the treatment of vascular spiders and cherry angiomas". Clinical and Experimental Dermatology. 28 (6): 581–3. doi:10.1046/j.1365-2230.2003.01352.x. PMID 14616818.
- Fodor, Lucian; Ramon, Ytzhack; Fodor, Adriana; Carmi, Nurit; Peled, Isaac J.; Ullmann, Yehuda (2006). "A Side-by-Side Prospective Study of Intense Pulsed Light and Nd:YAG Laser Treatment for Vascular Lesions". Annals of Plastic Surgery. 56 (2): 164–70. doi:10.1097/01.sap.0000196579.14954.d6. PMID 16432325.
- Lee, KW; Kang, NJ; Rogozin, EA; Kim, HG; Cho, YY; Bode, AM; Lee, HJ; Surh, YJ; et al. (2007). "Myricetin is a novel natural inhibitor of neoplastic cell transformation and MEK1". Carcinogenesis. 28 (9): 1918–27. doi:10.1093/carcin/bgm110. PMID 17693661.
- Kim, JE; Kwon, JY; Lee, DE; Kang, NJ; Heo, YS; Lee, KW; Lee, HJ (2009). "MKK4 is a novel target for the inhibition of tumor necrosis factor-alpha-induced vascular endothelial growth factor expression by myricetin". Biochemical pharmacology. 77 (3): 412–21. doi:10.1016/j.bcp.2008.10.027. PMID 19026990.
- Perkins, Sharon. "Cherry Angioma & Skin Cancer". livestrong.com. Retrieved 10 April 2018.
External links
| Classification | |
|---|---|
| External resources |
- eMedicine with picture showing small red dots
- Pereira, José Marcos (2004). "Hemangioma rubi no couro cabeludo". Anais Brasileiros de Dermatologia. 79: 83–89. doi:10.1590/S0365-05962004000100010.