CAD/CAM dentistry
CAD/CAM dentistry is a field of dentistry and prosthodontics using CAD/CAM (computer-aided design and computer-aided manufacturing) to improve the design and creation of dental restorations,[1][2] especially dental prostheses, including crowns, crown lays, veneers, inlays and onlays, fixed dental prostheses bridges, dental implant supported restorations, dentures (removable or fixed), and orthodontic appliances. CAD/CAM technology allows the delivery of a well-fitting, aesthetic, and a durable prostheses for the patient.[3] CAD/CAM complements earlier technologies used for these purposes by any combination of increasing the speed of design and creation; increasing the convenience or simplicity of the design, creation, and insertion processes; and making possible restorations and appliances that otherwise would have been infeasible. Other goals include reducing unit cost and making affordable restorations and appliances that otherwise would have been prohibitively expensive. However, to date, chairside CAD/CAM often involves extra time on the part of the dentist, and the fee is often at least two times higher than for conventional restorative treatments using lab services. CAD/CAM is one of the highly competent dental lab technologies.[4]

Like other CAD/CAM fields, CAD/CAM dentistry uses subtractive processes (such as CNC milling) and additive processes (such as 3D printing) to produce physical instances from 3D models.
In some cases, “CAD/CAM” in dental technology is used to describe protheses made by milling technology but this is not fully correct as the term “CAD/CAM” does not relate to the method of production.[5]
History
Although CAD/CAM dentistry was used in the mid-1980s, early efforts were considered a cumbersome novelty, requiring an inordinate amount of time to produce a viable product. This inefficiency prevented its use within dental offices and limited it to labside use (that is, used within dental laboratories). As adjunctive techniques, software, and materials improved, the chairside use of CAD/CAM (use within dental offices/surgeries) increased.[6] For example, the commercialization of Cerec by Sirona made CAD/CAM available to dentists who formerly would not have had avenues for using it.
The article CEREC CAD/CAM in Dentistry[7] original dissertation Data capture stabilizing device for the CEREC CAD/CAM chairside camera[8] fully explains all pros and cons of the system and is detailed in (materials, fit, software, hardware, etc.).
Difference from conventional restoration
Chairside CAD/CAM restoration differs from conventional dentistry in that the prosthesis is typically luted or bonded the same day. Conventional prosthesis, such as crowns, have temporaries placed from one to several weeks while a dental laboratory or in house dental lab produces the restoration.[9] The patient returns later to have the temporaries removed and the laboratory-made crown cemented or bonded in place. An in-house CAD/CAM system enables the dentist to create a finished inlay in as little as an hour in some cases.[10] CAD/CAM systems use an optical camera to take a virtual impression by creating a 3D image which is forwarded to a software program and the impression results in a computer-generated cast on which the restoration is designed.[11]
Bonded veneer CAD/CAM restorations are more conservative in their preparation of the tooth. As bonding is more effective on tooth enamel than the underlying dentin, care is taken not to remove the enamel layer. Though one-day service is a benefit that is typically claimed by dentists offering chairside CAD/CAM services, the dentist's time is commonly doubled and the fee is therefore doubled.
Process
All CAD/CAM systems contain
- An optical scanner that captures the intraoral or extraoral condition
- Software that can turn the captured images into a digital model to produce and design the prosthesis
- Technology that changes the data into a product[5] As in other fields, additive manufacturing (3D printing) first entered CAD/CAM dentistry in the form of laboratory experiments, but its use has since expanded; and chairside use, although not yet widespread, is advancing
Typically CAD/CAM dental restorations are milled from solid blocks of ceramic or composite resin that closely match the basic shade of the restored tooth. Metal alloys, including zirconia, can also be milled.
Several of these materials require processing such as baking or sintering following their milling. The system can be used chair-side, in a laboratory setting, or in a production centre.[5]
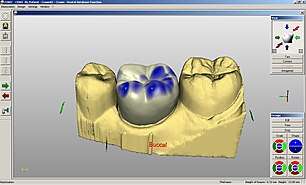
For a single unit prosthesis, after decayed or broken areas of the tooth are corrected by the dentist, an optical impression is made of the prepared tooth and the surrounding teeth. These images are then turned into a digital model by proprietary software within which the prosthesis is created virtually. The software sends this data to a milling machine where the prosthesis is milled. Stains and glazes can be added to the surfaces of the milled ceramic crown or bridge to correct the otherwise monochromatic appearance of the restoration. The restoration is then adjusted in the patient’s mouth and luted or bonded in place.
Integrating optical scan data with cone beam computed tomography datasets within implantology software also enables surgical teams to digitally plan implant placement and fabricate a surgical guide for precise implementation of that plan. Combining CAD/CAM software with 3D images from 3D imaging system means greater safety and security from any kind of intraoperative mistakes.
Advantages and Drawbacks
CAD/CAM has improved the quality of prostheses in dentistry and found a way to standardise the production process. It has increased productivity and the chance to work with new materials with a high level of accuracy.[5] It has also found a way to decrease chair time for the patient by the use of intra-oral scanning systems which allow the dentist to send electronic impressions to the lab.[12] The restorations are milled from a block of ceramic which has fewer flaws.[13]
However, CAD/CAM requires a large initial outlay (expensive to buy) and occlusal detail isn't always the best and has to be amended by hand.[13] Most doctors that utilize the chair side technology find the level of detail to be more than adequate in a clinical setting.
Despite the CAD/CAM being a major technological advancement, it is important that the dentists’ technique is suited to the methods of CAD/CAM and milling technology. This includes: correct tooth preparations with a continuous preparation margin (which is recognisable to the scanner e.g. in the form of a chamfer); avoiding the use of shoulderless preparations and parallel walls and the use of rounded incisor and occlusal edges to prevent the concentration of tension.[5]
Depending on the material chosen, CAD/CAM treatments may have some aesthetic drawbacks, whether they are created at the dental practice or outsourced to a dental laboratory fabricating service. Depending on the dentist or technician, CAD/CAM restorations can be layered to give a deeper more natural look. Just like traditional restorations, CAD/CAM restorations also vary in aesthetic value, many are monochrome.[13] In some hand-layered crowns and bridges, feldspathic porcelain is fused to glass-infiltrated aluminum oxide (alumina) or zirconium-oxide (zirconia) creating a high-strength, highly aesthetic, metal-free crown or bridge. In other traditional restorations, this porcelain is layered onto a metal substructure and often display colour brightness, an opaque "headlight", and dark oxide lines (a "black line" in the vicinity of the gum line). As these dark metal substructures are not conducive to a natural appearance, metal-free restorations are typically more aesthetically pleasing to the patient.[14]
There are also different medical repercussions for each restorative technique. If the CAD/CAM restorative material is zirconia, the restoration becomes "radio-opaque", just as metal restorations are, blocking x-rays. Only alumina, lithium disilicate materials are "radio-lucent", allowing dentists to track potential decay. Zirconia, conventional porcelain-to-metal, and traditional gold and other all-metal crowns block x-ray radiation, disallowing evaluation over time. Therefore, doctors have to examine restorations visually and with a dental explorer to diagnose decay.
Crowns and bridges require an extremely precise fit on tooth abutments or stumps. Fit accuracy varies according to the CAD/CAD system utilized and from user to user. Some systems are designed to attain higher standards of accuracy than others and some users are more skilled than others. It is estimated that 20 new systems are expected to become available in the next five years.[15]
Further high quality research is needed to evaluate CAD/CAM technology compared to the numerous other attachment systems (such as ball, magnetic and telescopic systems), as an option for attaching overdentures to implants.[16]
References
- Davidowitz G, Kotick PG. (2011), "The use of CAD/CAM in dentistry.", Dent Clin North Am, 55 (3): 559–570, doi:10.1016/j.cden.2011.02.011, PMID 21726690.
- Rekow D (1987), "Computer-aided design and manufacturing in dentistry: a review of the state of the art", J Prosthet Dent, 58 (4): 512–516, doi:10.1016/0022-3913(87)90285-X, PMID 3312586.
- Oen, Kay T; Veitz-Keenan, Analia; Spivakovsky, Silvia; Wong, Y Jo; Bakarman, Eman; Yip, Julie (April 9, 2014). "CAD/CAM versus traditional indirect methods in the fabrication of inlays, onlays, and crowns". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.cd011063. ISSN 1465-1858.
- Charles Brown. "Which is the Highly Competent Dental Lab Technology Use Today". Archived from the original on September 29, 2015. Retrieved March 20, 2016. Cite journal requires
|journal=(help) - Edelhoff, D.; Schweiger, J.; Beuer, F. (May 2008). "Digital dentistry: an overview of recent developments for CAD/CAM generated restorations". British Dental Journal. 204 (9): 505–511. doi:10.1038/sj.bdj.2008.350. ISSN 1476-5373. PMID 18469768.
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. (January 2009). "A review of dental CAD/CAM: current status and future perspectives from 20 years of experience". Dent Mater Journal. 28 (1): 44–56. doi:10.4012/dmj.28.44. PMID 19280967.
- "CEREC CAD/CAM in Dentistry". May 29, 2015. Retrieved March 20, 2016. Cite journal requires
|journal=(help) - "Data capture stabilising device for the CEREC Cad/Cam chairside camera". April 9, 2010. Retrieved March 20, 2016. Cite journal requires
|journal=(help) - Masek, R. (January 2005). "Margin isolation for optical impressions and adhesion". International Journal of Computer Dentistry. 8 (1): 69–76. PMID 15892526.
- "CAD/CAM Technology: You Can't Afford NOT to Have It". Sidekick Magazine. Archived from the original on December 13, 2012. Retrieved March 20, 2016.
- Oen, Kay T; Veitz-Keenan, Analia; Spivakovsky, Silvia; Wong, Y Jo; Bakarman, Eman; Yip, Julie (April 9, 2014). "CAD/CAM versus traditional indirect methods in the fabrication of inlays, onlays, and crowns". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.cd011063. ISSN 1465-1858.
- Birnbaum, Nathan S.; Aaronson, Heidi B. (2018), "Digital Impression Devices and CAD/CAM Systems", Ronald E. Goldstein's Esthetics in Dentistry, John Wiley & Sons, Ltd, pp. 1386–1407, doi:10.1002/9781119272946.ch46, ISBN 9781119272946
- Principles of operative dentistry. Qualtrough, A. J. E. Oxford, UK: Blackwell Pub. 2005. ISBN 9781405118217. OCLC 56956075.CS1 maint: others (link)
- Masek, R. (July 1999). "Reproducing natural color effects on milled ceramic restorations". International Journal of Computer Dentistry. 2 (3): 209–17. PMID 11351485.
- Oen, Kay T; Veitz-Keenan, Analia; Spivakovsky, Silvia; Wong, Y Jo; Bakarman, Eman; Yip, Julie (April 9, 2014). "CAD/CAM versus traditional indirect methods in the fabrication of inlays, onlays, and crowns". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.cd011063. ISSN 1465-1858.
- Payne, Alan GT; Alsabeeha, Nabeel HM; Atieh, Momen A; Esposito, Marco; Ma, Sunyoung; Anas El-Wegoud, Marwah (October 11, 2018). "Interventions for replacing missing teeth: attachment systems for implant overdentures in edentulous jaws". Cochrane Database of Systematic Reviews. 10: CD008001. doi:10.1002/14651858.cd008001.pub2. ISSN 1465-1858. PMC 6516946. PMID 30308116.