Athlete's foot
Athlete's foot, known medically as tinea pedis, is a common skin infection of the feet caused by fungus.[2] Signs and symptoms often include itching, scaling, cracking and redness.[3] In rare cases the skin may blister.[6] Athlete's foot fungus may infect any part of the foot, but most often grows between the toes.[3] The next most common area is the bottom of the foot.[6] The same fungus may also affect the nails or the hands.[4] It is a member of the group of diseases known as tinea.[7]
| Athlete's foot | |
|---|---|
| Other names | Tinea pedis, ringworm of the foot,[1] moccasin foot[2] |
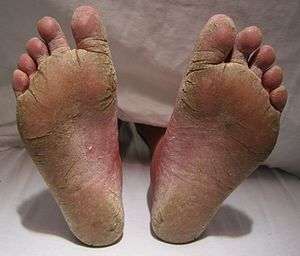 | |
| A severe case of athlete's foot | |
| Specialty | Infectious disease |
| Symptoms | Itching, scaling, redness of the foot[3] |
| Causes | Fungi (Trichophyton, Epidermophyton, Microsporum)[4] |
| Diagnostic method | Based on symptoms, confirmed by culture or microscopy[4] |
| Prevention | Avoiding walking barefoot in public showers, keeping toenails short, wearing big enough shoes, changing socks daily[4][5] |
| Treatment | Antifungal medication applied to the skin or taken by mouth[2][4] |
| Frequency | 15% of the population[2] |
Athlete's foot is caused by a number of different fungi,[3] including species of Trichophyton, Epidermophyton, and Microsporum.[4] The condition is typically acquired by coming into contact with infected skin, or fungus in the environment.[3] Common places where the fungi can survive are around swimming pools and in locker rooms.[8] They may also be spread from other animals.[5] Usually diagnosis is made based on signs and symptoms; however, it can be confirmed either by culture or seeing hyphae using a microscope.[4]
Some methods of prevention include avoiding walking barefoot in public showers, keeping the toenails short, wearing big enough shoes, and changing socks daily.[4][5] When infected, the feet should be kept dry and clean and wearing sandals may help.[3] Treatment can be either with antifungal medication applied to the skin such as clotrimazole or for persistent infections antifungal medication that are taken by mouth such as terbinafine.[2][4] The use of the cream is typically recommended for four weeks.[4]
Athlete's foot was first medically described in 1908.[9] Globally, athlete's foot affects about 15% of the population.[2] Males are more often affected than females.[4] It occurs most frequently in older children or younger adults.[4] Historically it is believed to have been a rare condition, that became more frequent in the 1900s due to the greater use of shoes, health clubs, war, and travel.[10]
Signs and symptoms

Athlete's foot is divided into four categories or presentations: chronic interdigital athlete's foot, plantar (chronic scaly) athlete's foot (aka "moccasin foot"), acute ulcerative tinea pedis,[11] and vesiculobullous athlete's foot.[2][12][13] "Interdigital" means between the toes. "Plantar" here refers to the sole of the foot. The ulcerative condition includes macerated lesions with scaly borders.[11] Maceration is the softening and breaking down of skin due to extensive exposure to moisture. A vesiculobullous disease is a type of mucocutaneous disease characterized by vesicles and bullae (blisters). Both vesicles and bullae are fluid-filled lesions, and they are distinguished by size (vesicles being less than 5–10 mm and bulla being larger than 5–10 mm, depending upon what definition is used).
Athlete's foot occurs most often between the toes (interdigital), with the space between the fourth and fifth digits most commonly afflicted.[14][15][16] Cases of interdigital athlete's foot caused by Trichophyton rubrum may be symptomless, it may itch, or the skin between the toes may appear red or ulcerative (scaly, flaky, with soft and white if skin has been kept wet),[7][17] with or without itching. An acute ulcerative variant of interdigital athlete's foot caused by T. mentagrophytes is characterized by pain, maceration of the skin, erosions and fissuring of the skin, crusting, and an odor due to secondary bacterial infection.[13]
Plantar athlete's foot (moccasin foot) is also caused by T. rubrum which typically causes asymptomatic, slightly erythematous plaques (areas of redness of the skin) to form on the plantar surface (sole) of the foot that are often covered by fine, powdery hyperkeratotic scales.[2][13]
The vesiculobullous type of athlete's foot is less common and is usually caused by T. mentagrophytes and is characterized by a sudden outbreak of itchy blisters and vesicles on an erythematous base,[7] usually appearing on the sole of the foot. This subtype of athlete's foot is often complicated by secondary bacterial infection by Streptococcus pyogenes or Staphylococcus aureus.[13]
Complications
As the disease progresses, the skin may crack, leading to bacterial skin infection[13] and inflammation of the lymphatic vessels.[11] If allowed to grow for too long, athlete's foot fungus may spread to infect the toenails,[18] feeding on the keratin in them, a condition called onychomycosis.[19]
Because athlete's foot may itch, it may also elicit the scratch reflex, causing the host to scratch the infected area before they realize it. Scratching can further damage the skin and worsen the condition by allowing the fungus to more easily spread and thrive. The itching sensation associated with athlete's foot can be so severe that it may cause hosts to scratch vigorously enough to inflict excoriations (open wounds), which are susceptible to bacterial infection. Further scratching may remove scabs, inhibiting the healing process.
Scratching infected areas may also spread the fungus to the fingers and under the fingernails. If not washed away soon enough, it can infect the fingers and fingernails, growing in the skin and in the nails (not just underneath). After scratching, it can be spread to wherever the person touches, including other parts of the body and to one's environment. Scratching also causes infected skin scales to fall off into one's environment, leading to further possible spread.
When athlete's foot fungus or infested skin particles spread to one's environment (such as to clothes, shoes, bathroom, etc.) whether through scratching, falling, or rubbing off, not only can they infect other people, they can also reinfect (or further infect) the host they came from. For example, infected feet infest one's socks and shoes which further expose the feet to the fungus and its spores when worn again.
The ease with which the fungus spreads to other areas of the body (on one's fingers) poses another complication. When the fungus is spread to other parts of the body, it can easily be spread back to the feet after the feet have been treated. And because the condition is called something else in each place it takes hold (e.g., tinea corporis (ringworm) or tinea cruris (jock itch), persons infected may not be aware it is the same disease.
Some individuals may experience an allergic response to the fungus called an id reaction in which blisters or vesicles can appear in areas such as the hands, chest, and arms.[20] Treatment of the underlying infection typically results in the disappearance of the id reaction.[20]
Causes
Athlete's foot is a form of dermatophytosis (fungal infection of the skin), caused by dermatophytes, fungi (most of which are mold) which inhabit dead layers of skin and digest keratin.[2] Dermatophytes are anthropophilic, meaning these parasitic fungi prefer human hosts. Athlete's foot is most commonly caused by the molds known as Trichophyton rubrum and T. mentagrophytes,[21] but may also be caused by Epidermophyton floccosum.[22][23] Most cases of athlete's foot in the general population are caused by T. rubrum; however, the majority of athlete's foot cases in athletes are caused by T. mentagrophytes.[13]
Transmission
According to the UK's National Health Service, "Athlete’s foot is very contagious and can be spread through direct and indirect contact."[24] The disease may spread to others directly when they touch the infection. People can contract the disease indirectly by coming into contact with contaminated items (clothes, towels, etc.) or surfaces (such as bathroom, shower, or locker room floors). The fungi that cause athlete's foot can easily spread to one's environment. Fungi rub off of fingers and bare feet, but also travel on the dead skin cells that continually fall off the body. Athlete's foot fungi and infested skin particles and flakes may spread to socks, shoes, clothes, to other people, pets (via petting), bed sheets, bathtubs, showers, sinks, counters, towels, rugs, floors, and carpets.
When the fungus has spread to pets, it can subsequently spread to the hands and fingers of people who pet them. If a pet frequently gnaws upon itself, it might not be fleas it is reacting to, it may be the insatiable itch of tinea.
One way to contract athlete's foot is to get a fungal infection somewhere else on the body first. The fungi causing athlete's foot may spread from other areas of the body to the feet, usually by touching or scratching the affected area, thereby getting the fungus on the fingers, and then touching or scratching the feet. While the fungus remains the same, the name of the condition changes based on where on the body the infection is located. For example, the infection is known as tinea corporis ("ringworm") when the torso or limbs are affected or tinea cruris (jock itch or dhobi itch) when the groin is affected. Clothes (or shoes), body heat, and sweat can keep the skin warm and moist, just the environment the fungus needs to thrive.
Risk factors
Besides being exposed to any of the modes of transmission presented above, there are additional risk factors that increase one's chance of contracting athlete's foot. Persons who have had athlete's foot before are more likely to become infected than those who have not. Adults are more likely to catch athlete's foot than children. Men have a higher chance of getting athlete's foot than women.[25] People with diabetes or weakened immune systems[25] are more susceptible to the disease. HIV/AIDS hampers the immune system and increases the risk of acquiring athlete's foot. Hyperhidrosis (abnormally increased sweating) increases the risk of infection and makes treatment more difficult.[26]
Diagnosis

When visiting a doctor, the basic diagnosis procedure applies. This includes checking the patient's medical history and medical record for risk factors,[11] a medical interview during which the doctor asks questions (such as about itching and scratching), and a physical examination.[11] Athlete's foot can usually be diagnosed by visual inspection of the skin and by identifying less obvious symptoms such as itching of the affected area.
If the diagnosis is uncertain, direct microscopy of a potassium hydroxide preparation of a skin scraping (known as a KOH test) can confirm the diagnosis of athlete's foot and help rule out other possible causes, such as candidiasis, pitted keratolysis, erythrasma, contact dermatitis, eczema, or psoriasis.[13][23][27] Dermatophytes known to cause athlete's foot will demonstrate multiple septate branching hyphae on microscopy.[13]
A Wood's lamp (black light), although useful in diagnosing fungal infections of the scalp (tinea capitis), is not usually helpful in diagnosing athlete's foot, since the common dermatophytes that cause this disease do not fluoresce under ultraviolet light.[14]
Prevention
There are several preventive foot hygiene measures that can prevent athlete's foot and reduce recurrence. Some of these include keeping the feet dry, clipping toenails short; using a separate nail clipper for infected toenails; using socks made from well-ventilated cotton or synthetic moisture wicking materials (to soak moisture away from the skin to help keep it dry); avoiding tight-fitting footwear, changing socks frequently; and wearing sandals while walking through communal areas such as gym showers and locker rooms.[8][13][28]
According to the Centers for Disease Control and Prevention, "Nails should be clipped short and kept clean. Nails can house and spread the infection."[29] Recurrence of athlete's foot can be prevented with the use of antifungal powder on the feet.[13]
The fungi (molds) that cause athlete's foot require warmth and moisture to survive and grow. There is an increased risk of infection with exposure to warm, moist environments (e.g., occlusive footwear—shoes or boots that enclose the feet) and in shared humid environments such as communal showers, shared pools, and treatment tubs.[17] Chlorine bleach is a disinfectant and common household cleaner that kills mold. Cleaning surfaces with a chlorine bleach solution prevents the disease from spreading from subsequent contact. Cleaning bathtubs, showers, bathroom floors, sinks, and counters with bleach helps prevent the spread of the disease, including reinfection.
Keeping socks and shoes clean (using bleach in the wash) is one way to prevent fungi from taking hold and spreading. Avoiding the sharing of boots and shoes is another way to prevent transmission. Athlete's foot can be transmitted by sharing footwear with an infected person. Hand-me-downs and purchasing used shoes are other forms of shoe-sharing. Not sharing also applies to towels, because, though less common, fungi can be passed along on towels, especially damp ones.
Treatment
Athlete's foot resolves without medication (resolves by itself) in 30–40% of cases.[30] Topical antifungal medication consistently produce much higher rates of cure.[31]
Conventional treatment typically involves thoroughly washing the feet daily or twice daily, followed by the application of a topical medication. Because the outer skin layers are damaged and susceptible to reinfection, topical treatment generally continues until all layers of the skin are replaced, about 2–6 weeks after symptoms disappear. Keeping feet dry and practising good hygiene (as described in the above section on prevention) is crucial for killing the fungus and preventing reinfection.
Treating the feet is not always enough. Once socks or shoes are infested with fungi, wearing them again can reinfect (or further infect) the feet. Socks can be effectively cleaned in the wash by adding bleach or by washing in water 60 °C (140 °F).[32] Washing with bleach may help with shoes, but the only way to be absolutely certain that one cannot contract the disease again from a particular pair of shoes is to dispose of those shoes.
To be effective, treatment includes all infected areas (such as toenails, hands, torso, etc.). Otherwise, the infection may continue to spread, including back to treated areas. For example, leaving fungal infection of the nail untreated may allow it to spread back to the rest of the foot, to become athlete's foot once again.
Allylamines such as terbinafine are considered more efficacious than azoles for the treatment of athlete's foot.[13][33]
Severe or prolonged fungal skin infections may require treatment with oral antifungal medication.
Topical treatments
There are many topical antifungal drugs useful in the treatment of athlete's foot including: miconazole nitrate, clotrimazole, tolnaftate (a synthetic thiocarbamate), terbinafine hydrochloride,[17] butenafine hydrochloride and undecylenic acid. The fungal infection may be treated with topical antifungal agents, which can take the form of a spray, powder, cream, or gel. Topical application of an antifungal cream such as butenafine once daily for one week or terbinafine once daily for two weeks is effective in most cases of athlete's foot and is more effective than application of miconazole or clotrimazole.[23] Plantar-type athlete's foot is more resistant to topical treatments due to the presence of thickened hyperkeratotic skin on the sole of the foot.[13] Keratolytic and humectant medications such as urea, salicyclic acid (Whitfield's ointment), and lactic acid are useful adjunct medications and improve penetration of antifungal agents into the thickened skin.[13] Topical glucocorticoids are sometimes prescribed to alleviate inflammation and itching associated with the infection.[13]
A solution of 1% potassium permanganate dissolved in hot water is an alternative to antifungal drugs.[34] Potassium permanganate is a salt and a strong oxidizing agent.
Oral treatments
For severe or refractory cases of athlete's foot oral terbinafine is more effective than griseofulvin.[2] Fluconazole or itraconazole may also be taken orally for severe athlete's foot infections.[2] The most commonly reported adverse effect from these medications is gastrointestinal upset.[2]
Epidemiology
Globally, fungal infections affect about 15% of the population and 20% of adults.[2][21] Athlete's foot is common in individuals who wear unventilated (occlusive) footwear, such as rubber boots or vinyl shoes.[21][23] Countries and regions where going barefoot is more common experience much lower rates of athlete's foot than do populations which habitually wear shoes; as a result, the disease has been called "a penalty of civilization".[35] Studies have demonstrated that men are infected 2–4 times more often than women.[2]
See also
- Toenail fungus, tinea unguium, an infection affecting the toenails
- Trench foot
References
- Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. p. 1135. ISBN 978-1-4160-2999-1.
- Bell-Syer, SE; Khan, SM; Torgerson, DJ (17 October 2012). Bell-Syer, Sally EM (ed.). "Oral treatments for fungal infections of the skin of the foot" (PDF). The Cochrane Database of Systematic Reviews. 10: CD003584. doi:10.1002/14651858.CD003584.pub2. PMID 23076898.
- "Hygiene-related Diseases". CDC. 24 December 2009. Archived from the original on 30 January 2016. Retrieved 24 January 2016.
- Kaushik, N; Pujalte, GG; Reese, ST (December 2015). "Superficial Fungal Infections". Primary Care. 42 (4): 501–16. doi:10.1016/j.pop.2015.08.004. PMID 26612371.
- "People at Risk for Ringworm". CDC. 6 December 2015. Archived from the original on 7 September 2016.
- "Symptoms of Ringworm". CDC. 6 December 2015. Archived from the original on 20 January 2016. Retrieved 24 January 2016.
- Moriarty, B; Hay, R; Morris-Jones, R (July 2012). "The diagnosis and management of tinea". BMJ. 345 (7): e4380. doi:10.1136/bmj.e4380. PMID 22782730.
- Hawkins, DM; Smidt, AC (April 2014). "Superficial fungal infections in children". Pediatric Clinics of North America. 61 (2): 443–55. doi:10.1016/j.pcl.2013.12.003. PMID 24636655.
- Homei, Aya; Worboys, Michael (2013). Fungal disease in Britain and the United States 1850-2000 : mycoses and modernity. p. 44. ISBN 9781137377036. Archived from the original on 30 January 2016.
- Perfect, edited by Mahmoud A. Ghannoum, John R. (2009). Antifungal Therapy. New York: Informa Healthcare. p. 258. ISBN 9780849387869. Archived from the original on 30 January 2016.CS1 maint: extra text: authors list (link)
- The Merck Manual Professional Edition tinea pedis page Archived 28 January 2015 at the Wayback Machine. Retrieved 16 January 2015.
- "Athlete's Foot". Archived from the original on 6 December 2010. Retrieved 26 May 2010.
- TIougan, BE; Mancini, AJ; Mandell, JA; Cohen, DE; Sanchez, MR (November 2011). "Skin conditions in figure skaters, ice-hockey players and speed skaters: part II – cold-induced, infectious and inflammatory dermatoses". Sports Medicine. 41 (11): 967–984. doi:10.2165/11592190-000000000-00000. PMID 21985216.
- Al Hasan M; Fitzgerald SM; Saoudian M; Krishnaswamy G (2004). "Dermatology for the practicing allergist: Tinea pedis and its complications". Clinical and Molecular Allergy. 2 (1): 5. doi:10.1186/1476-7961-2-5. PMC 419368. PMID 15050029.
- Hainer BL (2003). "Dermatophyte infections". American Family Physician. 67 (1): 101–8. PMID 12537173.
- Hirschmann JV; Raugi GJ (2000). "Pustular tinea pedis". Journal of the American Academy of Dermatology. 42 (1 Pt 1): 132–133. doi:10.1016/S0190-9622(00)90022-7. PMID 10607333.
- Likness, LP (June 2011). "Common dermatologic infections in athletes and return-to-play guidelines". The Journal of the American Osteopathic Association. 111 (6): 373–379. doi:10.7556/jaoa.2011.111.6.373. PMID 21771922.
- National Health Service webpage on Athlete's Foot Archived 14 January 2015 at the Wayback Machine. Retrieved 14 January 2015.
- Flint, WW; Cain, JD (March 2014). "Nail and skin disorders of the foot". The Medical Clinics of North America. 98 (2): 213–25. doi:10.1016/j.mcna.2013.11.002. PMID 24559870.
- Ilkit, M; Durdu, M; Karakaş, M (August 2012). "Cutaneous id reactions: a comprehensive review of clinical manifestations, epidemiology, etiology, and management". Critical Reviews in Microbiology. 38 (3): 191–202. doi:10.3109/1040841X.2011.645520. PMID 22300403.
- Havlickova, B; Czaika, VA; Friedrich, M (September 2008). "Epidemiological trends in skin mycoses worldwide". Mycoses. 51 (Supplement 4): 2–15. doi:10.1111/j.1439-0507.2008.01606.x. PMID 18783559.
- Rivera, ZS; Losada, L; Nierman, WC (October 2012). "Back to the future for dermatophyte genomics". mBio. 3 (6): e00381–12. doi:10.1128/mBio.00381-12. PMC 3487774. PMID 23111872.
- Andrews, MD; Burns, M (May 2008). "Common tinea infections in children". American Family Physician. 77 (10): 1415–1420. PMID 18533375. Archived from the original on 9 November 2013.
- National Health Service's webpage on Athlete's Foot causes Archived 14 January 2015 at the Wayback Machine
- Mayo Clinic website, Athlete's Foot Risk Factors Archived 7 February 2015 at the Wayback Machine
- The Merck Manual Professional Edition. Tinea Pedis Archived 28 January 2015 at the Wayback Machine
- del Palacio, Amalia; Margarita Garau; Alba Gonzalez-Escalada & Mª Teresa Calvo. "Trends in the treatment of dermatophytosis" (PDF). Biology of Dermatophytes and Other Keratinophilic Fungi: 148–158. Archived (PDF) from the original on 10 July 2007. Retrieved 10 October 2007.
- De Luca, JF; Adams, BB; Yosipovitch, G (May 2012). "Skin manifestations of athletes competing in the summer olympics: what a sports medicine physician should know". Sports Medicine. 42 (5): 399–413. doi:10.2165/11599050-000000000-00000. PMID 22512412.
- Centers for Disease Control webpage on Athlete's Foot Archived 30 January 2016 at the Wayback Machine. Retrieved 11 January 2015.
- Over-the-Counter Foot Remedies Archived 29 September 2007 at the Wayback Machine (American Family Physician)
- Crawford F; Hollis S (18 July 2007). Crawford, Fay (ed.). "Topical treatments for fungal infections of the skin and nails of the foot" (Review). Cochrane Database of Systematic Reviews (3): CD001434. doi:10.1002/14651858.CD001434.pub2. PMID 17636672.
- "Archived copy" (PDF). Archived from the original (PDF) on 26 September 2017. Retrieved 25 September 2017.CS1 maint: archived copy as title (link)
- Rotta, I; Sanchez, A; Gonçalves, PR; Otuki, MF; Correr, CJ (May 2012). "Efficacy and safety of topical antifungals in the treatment of dermatomycosis: a systematic review". British Journal of Dermatology. 166 (5): 927–933. doi:10.1111/j.1365-2133.2012.10815.x. PMID 22233283.
- "Potassium Permanganate". Archived from the original on 14 May 2011. Retrieved 31 March 2011.
- Gill, David; Marks, Robin (1999). "A review of the epidemiology of tinea unguium in the community". Australas J Dermatol. 40 (1): 6–13. doi:10.1046/j.1440-0960.1999.00308.x. PMID 10098282.
External links

| Classification | |
|---|---|
| External resources |
| Authority control |
|
|---|