Angiotensin II receptor blocker
Angiotensin II receptor blockers (ARBs), also known as angiotensin II receptor antagonists, AT1 receptor antagonists or sartans, are a group of pharmaceuticals that modulate the renin–angiotensin system. Their main uses are in the treatment of hypertension (high blood pressure), diabetic nephropathy (kidney damage due to diabetes) and congestive heart failure. They selectively block the activation of AT1 receptors, preventing the binding of angiotensin II compared to ACE inhibitors.
ARBs and the similar-attributed ACE inhibitors are both indicated as the first-line antihypertensives in patients developing hypertension along the left-sided heart failure.[1] However, ARBs appear to produce less adverse effects compared to ACE inhibitors.[1]
Medical uses
Angiotensin II receptor blockers are used primarily for the treatment of hypertension where the patient is intolerant of ACE inhibitor therapy primarily because of cough.[2] They do not inhibit the breakdown of bradykinin or other kinins, and are thus only rarely associated with the persistent dry cough and/or angioedema that limit ACE inhibitor therapy. More recently, they have been used for the treatment of heart failure in patients intolerant of ACE inhibitor therapy, in particular candesartan. Irbesartan and losartan have trial data showing benefit in hypertensive patients with type II diabetes, and may delay the progression of diabetic nephropathy. A 1998 double-blind study found "that lisinopril improved insulin sensitivity whereas losartan did not affect it."[3] Candesartan is used experimentally in preventive treatment of migraine.[4][5] Lisinopril has been found less often effective than candesartan at preventing migraine.[6]
The angiotensin II receptor blockers have differing potencies in relation to blood pressure control, with statistically differing effects at the maximal doses.[7] When used in clinical practice, the particular agent used may vary based on the degree of response required.
Some of these drugs have a uricosuric effect.[8][9]
In one study after 10 weeks of treatment with an ARB called losartan (Cozaar), 88% of hypertensive males with sexual dysfunction reported improvement in at least one area of sexuality, and overall sexual satisfaction improved from 7.3% to 58.5%.[10] In a study comparing beta-blocker carvedilol with valsartan, the angiotensin II receptor blocker not only had no deleterious effect on sexual function, but actually improved it.[11] Other ARBs include candesartan (Atacand), telmisartan (Micardis), and Valsartan (Diovan), fimasartan (Kanarb).
Angiotensin II, through AT1 receptor stimulation, is a major stress hormone and, because (ARBs) block these receptors, in addition to their eliciting anti-hypertensive effects, may be considered for the treatment of stress-related disorders.[12]
In 2008, they were reported to have a remarkable negative association with Alzheimer's disease (AD). A retrospective analysis of five million patient records with the US Department of Veterans Affairs system found different types of commonly used antihypertensive medications had very different AD outcomes. Those patients taking angiotensin receptor blockers (ARBs) were 35–40% less likely to develop AD than those using other antihypertensives.[13][14]
Adverse effects
This class of drugs is usually well tolerated. Common adverse drug reactions (ADRs) include: dizziness, headache, and/or hyperkalemia. Infrequent ADRs associated with therapy include: first dose orthostatic hypotension, rash, diarrhea, dyspepsia, abnormal liver function, muscle cramp, myalgia, back pain, insomnia, decreased hemoglobin levels, renal impairment, pharyngitis, and/or nasal congestion.[15] A 2014 Cochrane systematic review based on randomized controlled trials reported that when comparing patients taking ACE inhibitors to patients taking ARBs, fewer ARB patients withdrew from the study due to adverse events compared to ACE inhibitor patients.[16]
While one of the main rationales for the use of this class is the avoidance of dry cough and/or angioedema associated with ACE inhibitor therapy, rarely they may still occur. In addition, there is also a small risk of cross-reactivity in patients having experienced angioedema with ACE inhibitor therapy.[15]
Myocardial infarction
The issue of whether angiotensin II receptor antagonists slightly increase the risk of myocardial infarction (MI or heart attack) is currently being investigated. Some studies suggest ARBs can increase the risk of MI.[17] However, other studies have found ARBs do not increase the risk of MI.[18] To date, with no consensus on whether ARBs have a tendency to increase the risk of myocardial infarction, further investigations are underway.
Indeed, as a consequence of AT1 blockade, ARBs increase angiotensin II levels several-fold above baseline by uncoupling a negative-feedback loop. Increased levels of circulating angiotensin II result in unopposed stimulation of the AT2 receptors, which are, in addition, upregulated. However, recent data suggest AT2 receptor stimulation may be less beneficial than previously proposed, and may even be harmful under certain circumstances through mediation of growth promotion, fibrosis, and hypertrophy, as well as eliciting proatherogenic and proinflammatory effects.[19][20][21]
Cancer
A study published in 2010 determined that "...meta-analysis of randomised controlled trials suggests that ARBs are associated with a modestly increased risk of new cancer diagnosis. Given the limited data, it is not possible to draw conclusions about the exact risk of cancer associated with each particular drug. These findings warrant further investigation." [22] A later meta-analysis by the U.S. Food and Drug Administration (FDA) of 31 randomized controlled trials comparing ARBs to other treatment found no evidence of an increased risk of incident (new) cancer, cancer-related death, breast cancer, lung cancer, or prostate cancer in patients receiving ARBs.[23] In 2013, comparative effectiveness research from the United States Department of Veterans Affairs on the experience of more than a million Veterans found no increased risks for either lung cancer [24] (original article in Journal of Hypertension) or prostate cancer.[25] The researchers concluded "In this large nationwide cohort of United States Veterans, we found no evidence to support any concern of increased risk of lung cancer among new users of ARBs compared with nonusers. Our findings were consistent with a protective effect of ARBs."[24]
In May 2013, a senior regulator at the Food & Drug Administration, Medical Team Leader Thomas A. Marciniak, revealed publicly that contrary to the FDA's official conclusion that there was no increased cancer risk, after a patient by patient examination of the available FDA data he had concluded that there was a lung-cancer risk increase of about 24% in ARB patients, compared with patients taking a placebo or other drugs. One of the criticisms Marciniak made was that the earlier FDA meta-analysis did not count lung carcinomas as cancers. In ten of the eleven studies he examined, Marciniak said that there were more lung cancer cases in the ARB group than the control group. Ellis Unger, chief of the drug-evaluation division that includes Dr. Marciniak, was quoted as calling the complaints a "diversion," and saying in an interview, "We have no reason to tell the public anything new." In an article about the dispute, the Wall Street Journal interviewed three other doctors to get their views; one had "no doubt" ARBs increased cancer risk, one was concerned and wanted to see more data, and the third thought there was either no relationship or a hard to detect, low-frequency relationship.[26]
A 2016 meta-analysis including 148,334 patients found no significant differences in cancer incidence associated with ARB use.[27]
Renal failure
ARB inhibitors, although have protective effects against developing kidney diseases for patients with diabetes and previously hypertension without administration of ARBs, may worsen kidney functions such as causing further reduction of glomerular filtration rate associated with rise of serum creatinine in patients suffering practically clinical or already clinically present proteinuria, renal artery stenosis, hypertensive nephrosclerosis, heart failure, polycystic kidney disease, chronic kidney disease, interstitial fibrosis, focal segmental glomerulosclerosis, or any conditions such as ARBs-treated but still clinically hypertension that lead to abnormal narrowing of blood vessels to the kidney that interrupts oxygen and nutrients supply to the organ.[28][29][30][31][32][33]
History
Structure
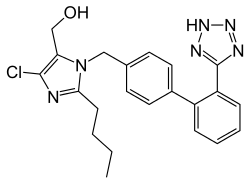
Losartan, irbesartan, olmesartan, candesartan, valsartan, fimasartan and azilsartan include the tetrazole group (a ring with four nitrogen and one carbon). Losartan, irbesartan, olmesartan, candesartan, and telmisartan include one or two imidazole groups.
Mechanism of action
These substances are AT1-receptor antagonists; that is, they block the activation of angiotensin II AT1 receptors. AT1 receptors are found in smooth muscle cells of vessels, cortical cells of the adrenal gland, and adrenergic nerve synapses. Blockage of AT1 receptors directly causes vasodilation, reduces secretion of vasopressin, and reduces production and secretion of aldosterone, among other actions. The combined effect reduces blood pressure.
The specific efficacy of each ARB within this class depends upon a combination of three pharmacodynamic (PD) and pharmacokinetic (PK) parameters. Efficacy requires three key PD/PK areas at an effective level; the parameters of the three characteristics will need to be compiled into a table similar to one below, eliminating duplications and arriving at consensus values; the latter are at variance now.
Pressor inhibition
Pressor inhibition at trough level - this relates to the degree of blockade or inhibition of the blood pressure-raising ("pressor") effect of angiotensin II. However, pressor inhibition is not a measure of blood pressure-lowering (BP) efficacy per se. The rates as listed in the U.S. Food and Drug Administration (FDA) Package Inserts (PIs) for inhibition of this effect at the 24th hour for the ARBs are as follows: (all doses listed in PI are included)
- Valsartan 80 mg 30%
- Telmisartan 80 mg 40%
- Losartan 100 mg 25–40%
- Irbesartan 150 mg 40%
- Irbesartan 300 mg 60%
- Azilsartan 32 mg 60%
- Olmesartan 20 mg 61%
- Olmesartan 40 mg 74%
AT1 affinity vs AT2
The ratios of AT1 to AT2 in binding affinities of the specific ARBs are shown as follows. Whereas, AT1 affinity vs AT2 is not a meaningful efficacy measurement of BP response.
- Losartan 1000-fold
- Telmisartan 3000-fold
- Irbesartan 8500-fold
- Candesartan greater than 10000-fold
- Olmesartan 12500-fold
- Valsartan 30000-fold higher than AT2 (The ratio of binding affinities of valsartan to AT1 and AT2 is 30000:1 ) [34][35]
- Saprisartan[36]
Binding affinities Ki
Component
Nearly all ARBs contain biphenyltetrazole moiety except telmisartan and eprosartan.[35]
Active agent
Losartan carries a heterocycle imidazole while valsartan carries a nonplanar acylated amino acid.[35]
Biological half-life
The third area needed to complete the overall efficacy picture of an ARB is its biological half-life. The half-lives from the U.S. Food and Drug Administration (FDA) Package Inserts (PIs) are as follows:
- Valsartan 6 hours
- Losartan 6–9 hours
- Azilsartan 11 hours
- Irbesartan 11–15 hours
- Olmesartan 13 hours
- Telmisartan 24 hours
- Fimasartan 7–11 hours
Comparison and pharmacokinetics
| Drug | Trade Name | Biological half-life [h] | Peak plasma concentration [Tmax] | Protein binding [%] | Bioavailability [%] | Renal/hepatic clearance [%] | Food effect | Daily dosage [mg] | Metabolism/transporter |
|---|---|---|---|---|---|---|---|---|---|
| Losartan | Cozaar | 6–9 h |
|
98.7% | 33% | 10/90% | Minimal | 50–100 mg | Sensitive substrates: CYP2C9 and CYP3A4[37] |
| EXP 3174 | 6–9 h | 99.8% | – | 50/50% | – | – | |||
| Candesartan | Atacand | 9h | 3-4 hrs[38] | >99% | 15% | 60/40% | No | 4–32 mg | Moderate sensitive substrate: CYP2C9[38] |
| Valsartan | Diovan | 6 h | 2-4 hrs[39] | 95% | 25% | 30/70% | No | 80–320 mg | Substrates:MRP2 and OATP1B1/SLCO1B1[39] |
| Irbesartan | Avapro | 11–15 h | 1.5 to 2 hrs[40] | 90–95% | 70% | 20/80% | No | 150–300 mg | Minor substrates of CYP2C9[40] |
| Telmisartan | Micardis | 24 h | 0.5 to 1 hour [41] | >99% | 42–58% | 1/99% | No | 40–80 mg | Unknown[41] |
| Eprosartan | Teveten | 5 h | 1 to 2 hours [42] | 98% | 13% | 30/70% | No | 400–800 mg | None known [42] |
| Olmesartan | Benicar/Olmetec | 14–16 h | 1 to 2 hours [43] | >99% | 29% | 40/60% | No | 10–40 mg | Substrates of OATP1B1/SLCO1B1[43] |
| Azilsartan | Edarbi | 11 h | 1.5 to 3 hours [44] | >99% | 60% | 55/42% | No | 40–80 mg | Minor substrates of CYP2C9 [44] |
| Fimasartan | Kanarb | 7–11 h | 30 mins to 3 hrs after dosing.[45] | >97% | 30–40% | - | - | 30–120 mg | No related research as of February 2019. |
Longevity promotion
Knockout of the Agtr1a gene that encodes AT1 results in marked prolongation of the life-span of mice by 26% compared to controls. The likely mechanism is reduction of oxidative damage (especially to mitochondria) and overexpression of renal prosurvival genes. The ARBs seem to have the same effect.[51][52]
Fibrosis regression
Losartan and other ARBs regress liver, heart, lung and kidney fibrosis.
Dilated aortic root regression
A 2003 study using candesartan and valsartan demonstrated an ability to regress dilated aortic root size.[53]
Recalls
In 2018 and in 2019, the U.S Food and Drug Administration (FDA) found traces of NDMA and NDEA impurities in the ARB drug products valsartan, losartan, and irbesartan.[54][55][56][57][58] The FDA stated "In June 2018, FDA was informed of the presence of an impurity, identified as N-Nitrosodimethylamine (NDMA), from one valsartan API producer. Since then, FDA has determined that other types of nitrosamine compounds, e.g., N-Nitrosodiethylamine (NDEA), are present at unacceptable levels in APIs from multiple API producers of valsartan and other drugs in the ARB class."[59] In 2018, the FDA issued guidance to the industry on how to assess and control the impurities.[60]
References
- "Management of Hypertension in Chronic Heart Failure". Today on Medscape. Retrieved 2019-02-03.
- "Choice of drug therapy in primary (essential) hypertension". UpToDate. Retrieved 2019-02-03.
- Fogari R, Zoppi A, Corradi L, Lazzari P, Mugellini A, Lusardi P (1998). "Comparative effects of lisinopril and losartan on insulin sensitivity in the treatment of non diabetic hypertensive patients". Br J Clin Pharmacol. 46 (5): 467–71. doi:10.1046/j.1365-2125.1998.00811.x. PMC 1873694. PMID 9833600.
- Tronvik E, Stovner LJ, Helde G, Sand T, Bovim G (2003). "Prophylactic treatment of migraine with an angiotensin II receptor blocker: a randomized controlled trial". JAMA. 289 (1): 65–69. doi:10.1001/jama.289.1.65. PMID 12503978.
- Cernes R, Mashavi M, Zimlichman R (2011). "Differential clinical profile of candesartan compared to other angiotensin receptor blockers". Vasc Health Risk Manag. 7: 749–59. doi:10.2147/VHRM.S22591. PMC 3253768. PMID 22241949.
- Gales BJ, Bailey EK, Reed AN, Gales MA (February 2010). "Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for the prevention of migraines". Ann Pharmacother. 44 (2): 360–66. doi:10.1345/aph.1M312. PMID 20086184.
- Kassler-Taub K, Littlejohn T, Elliott W, Ruddy T, Adler E (1998). "Comparative efficacy of two angiotensin II receptor antagonists, irbesartan and losartan in mild-to-moderate hypertension. Irbesartan/Losartan Study Investigators". Am J Hypertens. 11 (4 Pt 1): 445–53. doi:10.1016/S0895-7061(97)00491-3. PMID 9607383.
- Dang A, Zhang Y, Liu G, Chen G, Song W, Wang B (January 2006). "Effects of losartan and irbesartan on serum uric acid in hypertensive patients with hyperuricaemia in Chinese population". J Hum Hypertens. 20 (1): 45–50. doi:10.1038/sj.jhh.1001941. PMID 16281062.
- Daskalopoulou SS, Tzovaras V, Mikhailidis DP, Elisaf M (2005). "Effect on serum uric acid levels of drugs prescribed for indications other than treating hyperuricaemia". Curr. Pharm. Des. 11 (32): 4161–75. doi:10.2174/138161205774913309. PMID 16375738.
- Llisterri, JL; Lozano Vidal, JV; Aznar Vicente, J; Argaya Roca, M; Pol Bravo, C; Sanchez Zamorano, MA; Ferrario, CM (2001). "Sexual dysfunction in hypertensive patients treated with losartan". The American Journal of the Medical Sciences. 321 (5): 336–41. doi:10.1097/00000441-200105000-00006. PMID 11370797.
- Fogari, R; Zoppi, A; Poletti, L; Marasi, G; Mugellini, A; Corradi, L (2001). "Sexual activity in hypertensive men treated with valsartan or carvedilol: A crossover study". American Journal of Hypertension. 14 (1): 27–31. doi:10.1016/S0895-7061(00)01214-0. PMID 11206674.
- Pavel, J; Benicky, J; Murakami, I; Sanchez-Lemus, Y; Saavedra, E; Zhou, J; Saavedra, JM (2008). "Peripherally administered Angiotensin II AT1 receptor antagonists are anti-stress compounds in vivo". Annals of the New York Academy of Sciences. 1148 (1): 360–66. Bibcode:2008NYASA1148..360P. doi:10.1196/annals.1410.006. PMC 2659765. PMID 19120129.
- Li NC, Lee A, Whitmer RA, Kivipelto M, Lawler E, Kazis LE, Wolozin B (2010). "Use of angiotensin receptor blockers and risk of dementia in a predominantly male population: prospective cohort analysis". BMJ. 340 (9): b5465. doi:10.1136/bmj.b5465. PMC 2806632. PMID 20068258.
- "Potential of antihypertensive drugs for the prevention and treatment of Alzheimer's disease". Expert Review of Neurotherapeutics. 8 (9): 1285–1287. September 2008. doi:10.1586/14737175.8.9.1285.
- Rossi S, editor. Australian Medicines Handbook 2006. Adelaide: Australian Medicines Handbook; 2006.
- Li, Edmond CK; Heran, Balraj S; Wright, James M (2014). "Angiotensin converting enzyme (ACE) inhibitors versus angiotensin receptor blockers for primary hypertension". Cochrane Database of Systematic Reviews (8): CD009096. doi:10.1002/14651858.CD009096.pub2. PMC 6486121. PMID 25148386.
- Strauss MH, Hall AS (2006). "Angiotensin receptor blockers may increase risk of myocardial infarction: unraveling the ARB-MI paradox". Circulation. 114 (8): 838–54. doi:10.1161/CIRCULATIONAHA.105.594986. PMID 16923768.
- Tsuyuki RT, McDonald MA (2006). "Angiotensin receptor blockers do not increase risk of myocardial infarction". Circulation. 114 (8): 855–60. doi:10.1161/CIRCULATIONAHA.105.594978. PMID 16923769.
- Levy BI (2005). "How to explain the differences between renin angiotensin system modulators". Am. J. Hypertens. 18 (9 Pt 2): 134S–41S. doi:10.1016/j.amjhyper.2005.05.005. PMID 16125050.
- Lévy BI (2004). "Can angiotensin II type 2 receptors have deleterious effects in cardiovascular disease? Implications for therapeutic blockade of the renin–angiotensin system". Circulation. 109 (1): 8–13. doi:10.1161/01.CIR.0000096609.73772.C5. PMID 14707017.
- Reudelhuber TL (2005). "The continuing saga of the AT2 receptor: a case of the good, the bad, and the innocuous". Hypertension. 46 (6): 1261–62. doi:10.1161/01.HYP.0000193498.07087.83. PMID 16286568.
- Sipahi I; Debanne, SM; Rowland, DY; Simon, DI; Fang, JC (2010). "Angiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trials". Lancet Oncol. 11 (7): 627–36. doi:10.1016/S1470-2045(10)70106-6. PMC 4070221. PMID 20542468.
- "Angiotensin FDA Drug Safety Communication: No increase in risk of cancer with certain blood pressure drugs – Angiotensin Receptor Blockers (ARBs)". Food and Drug Administration (FDA). 2 June 2011. Archived from the original on 8 December 2011.
- Rao GA; Mann, JR; Shoaibi, A; Pai, SG; Bottai, M; Sutton, SS; Haddock, KS; Bennett, CL; Hebert, JR (2010). "Angiotensin receptor blockers: are they related to lung cancer?". J. Hypertens. 31 (8): 1669–75. doi:10.1097/HJH.0b013e3283621ea3. PMC 3879726. PMID 23822929.
- Rao GA; Mann, JR; Bottai, M; Uemura, H; Burch, JB; Bennett, CL; Haddock, KS; Hebert, JR (2013). "Angiotensin receptor blockers and risk of prostate cancer among United States veterans". J Clin Pharmacol. 53 (7): 773–78. doi:10.1002/jcph.98. PMC 3768141. PMID 23686462.
- Burton, Thomas M. (31 May 2013). "Dispute Flares Inside FDA Over Safety of Popular Blood-Pressure Drugs". The Wall Street Journal. Archived from the original on 15 February 2018. Retrieved 1 May 2018.
- Yi, Zhao Y. (12 Apr 2016). "Angiotensin II Receptor Blockers and Cancer Risk". Medicine. 95 (18): e3600. doi:10.1097/MD.0000000000003600. PMC 4863811. PMID 27149494.
- Toto, RD; Mitchell, HC; Lee, HC; Milam, C; Pettinger, WA (1991-10-01). "Reversible renal insufficiency due to angiotensin converting enzyme inhibitors in hypertensive nephrosclerosis". Annals of Internal Medicine. 115 (7): 513–9. doi:10.7326/0003-4819-115-7-513. PMID 1883120.
- Bakris, GL; Weir, MR (2000-03-13). "Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: is this a cause for concern?". Archives of Internal Medicine. 160 (5): 685–93. doi:10.1001/archinte.160.5.685. PMID 10724055.
- Remuzzi, G; Ruggenenti, P; Perico, N (2002-04-16). "Chronic renal diseases: renoprotective benefits of renin-angiotensin system inhibition". Annals of Internal Medicine. 136 (8): 604–15. doi:10.7326/0003-4819-136-8-200204160-00010. PMID 11955029.
- Sarafidis, Pantelis A.; Khosla, Nitin; Bakris, George L. (2007). "Antihypertensive Therapy in the Presence of Proteinuria". American Journal of Kidney Diseases. 49 (1): 12–26. doi:10.1053/j.ajkd.2006.10.014. PMID 17185142.
- Weir, Matthew R. (2002). "Progressive renal and cardiovascular disease: Optimal treatment strategies". Kidney International. 62 (4): 1482–1492. doi:10.1111/j.1523-1755.2002.kid591.x. PMID 12234333.
- "ACE Inhibitors and ARBs in Patients with Kidney Disease". Pharmacy Times. Retrieved 2019-02-05.
- Kjeldsen, Sverre E; Brunner, Hans R; McInnes, Gordon T; Stolt, Pelle (2005). "Valsartan in the treatment of hypertension". Aging Health. Future Medicine Ltd. 1 (1): 27–36. doi:10.2217/1745509x.1.1.27.
- Siragy, H (2002). "Angiotensin receptor blockers: how important is selectivity?". American Journal of Hypertension. 15 (11): 1006–1014. doi:10.1016/s0895-7061(02)02280-x. PMID 12441224.
- "Saprisartan". www.drugbank.ca. Archived from the original on 28 September 2016. Retrieved 1 May 2018.
- "LOSARTAN- losartan potassium tablet, film coated". DailyMed. 2018-12-26. Retrieved 2019-02-06.
12.3 Pharmacokinetics/ Absorption: Following oral administration, the systemic bioavailability of losartan is approximately 33%. Mean peak concentrations of losartan and its active metabolite are reached in 1 hour and in 3 to 4 hours, respectively. While maximum plasma concentrations of losartan and its active metabolite are approximately equal, the AUC (area under the curve) of the metabolite is about 4 times as great as that of losartan. A meal slows absorption of losartan and decreases its Cmax but has only minor effects on losartan AUC or on the AUC of the metabolite (≈10% decrease). The pharmacokinetics of losartan and its active metabolite are linear with oral losartan doses up to 200 mg and do not change over time.
- "CANDESARTAN - candesartan tablet". DailyMed. 2017-06-27. Retrieved 2019-02-06.
- "VALSARTAN - valsartan tablet". DailyMed. 2017-12-07. Retrieved 2019-02-06.
- "IRBESARTAN - irbesartan tablet". DailyMed. 2018-09-04. Retrieved 2019-02-06.
- "TELMISARTAN - telmisartan tablet". DailyMed. 2018-11-01. Retrieved 2019-02-06.
- "EPROSARTAN MESYLATE- eprosartan mesylate tablet, film coated". DailyMed. 2014-12-05. Retrieved 2019-02-06.
- "OLMESARTAN MEDOXOMIL - olmesartan medoxomil tablet, film coated". DailyMed. 2017-05-04. Retrieved 2019-02-06.
- "EDARBI- azilsartan kamedoxomil tablet". DailyMed. 2018-01-25. Retrieved 2019-02-06.
- Gu, N., Kim, B., Kyoung, S.L., Kim, S.E., Nam, W.S., Yoon, S.H., Cho, J., Shin, S., Jang, I., Yu, K. The Effect of Fimasartan, an Angiotensin Receptor Type 1 Blocker, on the Pharmacokinetics and Pharmacodynamics of Warfarin in Healthy Korean Male Volunteers: A One- Sequence, Two-Period Crossover Clinical Trial. (2012). Clinical Therapeutics. 34(7): 1592-1600.
- Burnier, M.; Brunner, H.R. (2000), "Angiotensin II receptor antagonists", Lancet, 355 (9204): 637–645, doi:10.1016/S0140-6736(99)10365-9, PMID 10696996
- Analogue-based Drug Discovery (Optimizing Antihypertensive Therapy by Angiotensin Receptor Blockers; Farsang, C., Fisher, J., p.157-167) Editors; Fischer, J., Ganellin, R. Wiley-VCH 2006. ISBN 978-3-527-31257-3
- Brousil, J.A.; Burke, J.M. (2003), "Olmesartan Medoxomil: An Angiotensin II-Receptor Blocker", Clinical Therapeutics, 25 (4): 1041–1055, doi:10.1016/S0149-2918(03)80066-8, PMID 12809956
- Brunner, H.R. (2002), "The new oral angiotensin II antagonist olmesartan medoxomil: a concise overview", Journal of Human Hypertension, 16 (2): 13–16, doi:10.1038/sj.jhh.1001391, PMID 11967728, ProQuest 219966061
- Zusman, R.M.; Jullien, V; Lemetayer, P; Jarnier, P; Clementy, J (1999), "Are There Differences Among Angiotensin Receptor Blockers?", American Journal of Hypertension, 12 (2 Pt 1): 231–235, doi:10.1016/S0895-7061(99)00116-8, PMID 10090354
- Benigni A, Corna D, Zoja C, Sonzogni A, Latini R, Salio M, Conti S, Rottoli D, Longaretti L, Cassis P, Morigi M, Coffman T, Remuzzi G (2009). "Disruption of the Ang II type 1 receptor promotes longevity in mice". J. Clin. Invest. 119 (3): 524–30. doi:10.1172/JCI36703. PMC 2648681. PMID 19197138.
- Cassis P, Conti S, Remuzzi G, Benigni A (January 2010). "Angiotensin receptors as determinants of life span". Pflügers Arch. 459 (2): 325–32. doi:10.1007/s00424-009-0725-4. PMID 19763608.
- Weinberg MS, Weinberg AJ, Cord RB, Martin H (1 May 2003). "P-609: Regression of dilated aortic roots using supramaximal and usual doses of angiotensin receptor blockers". American Journal of Hypertension. 16 (S1): 259A. doi:10.1016/S0895-7061(03)00782-9. ISSN 0895-7061.
In conclusion, we demonstrated regression of DAR using ARBs at moderate and supramaximal doses. Intensive ARB therapy offers a promise to reduce the natural progression of disease in patients with DARs.
- "FDA Updates and Press Announcements on Angiotensin II Receptor Blocker (ARB) Recalls (Valsartan, Losartan, and Irbesartan)". Food and Drug Administration (FDA). 20 August 2018. Retrieved 17 September 2019.
- "Statement on the agency's ongoing efforts to resolve safety issue with ARB medications". Food and Drug Administration (FDA). 28 August 2019. Retrieved 17 September 2019.
- "FDA's Assessment of Currently Marketed ARB Drug Products". Food and Drug Administration (FDA). 4 April 2019. Retrieved 17 September 2019.
- "Search List of Recalled Angiotensin II Receptor Blockers (ARBs) including Valsartan, Losartan and Irbesartan". Food and Drug Administration (FDA). 28 June 2019. Retrieved 17 September 2019.
- "Updated: Torrent Pharmaceuticals Limited Expands Voluntary Nationwide Recall of Losartan Potassium Tablets, USP and Losartan Potassium / Hydrochlorothiazide Tablets, USP". U.S. Food and Drug Administration. 23 September 2019. Retrieved 24 September 2019.
- "General Advice ARB" (PDF). Food and Drug Administration (FDA). Retrieved 17 September 2019.

- "M7(R1) Assessment and Control of DNA Reactive (Mutagenic) Impurities in Pharmaceuticals To Limit Potential Carcinogenic Risk" (PDF). Food and Drug Administration (FDA). 30 August 2018. Retrieved 17 September 2019. Lay summary.
External links
- Angiotensin+II+Type+1+Receptor+Blockers at the US National Library of Medicine Medical Subject Headings (MeSH)