Angelman syndrome
Angelman syndrome (AS) is a genetic disorder that mainly affects the nervous system.[2] Symptoms include a small head and a specific facial appearance, severe intellectual disability, developmental disability, speaking problems, balance and movement problems, seizures, and sleep problems.[2] Children usually have a happy personality and have a particular interest in water.[2] The symptoms generally become noticeable by one year of age.[2]
| Angelman syndrome | |
|---|---|
| Other names | Happy puppet syndrome[1] |
.png) | |
| A five-year-old girl with Angelman syndrome. Features shown include telecanthus, bilateral epicanthic folds, small head, wide mouth, and an apparently happy demeanor; hands with tapered fingers, abnormal creases and broad thumbs. | |
| Pronunciation |
|
| Specialty | Medical genetics |
| Symptoms | Delayed development, unusually happy, intellectual disability, speech problems, balance and movement problems, small head, seizures[2] |
| Usual onset | Noticeable by 6–12 months[2] |
| Causes | Genetic (new mutation)[2] |
| Diagnostic method | Based on symptoms, genetic testing[3] |
| Differential diagnosis | Cerebral palsy, autism, Rett Syndrome, Prader-Willi syndrome[3][4] |
| Treatment | Supportive care[3] |
| Prognosis | Nearly normal life expectancy[2] |
| Frequency | 1 in 12,000 to 20,000 people[2] |
Angelman syndrome is typically due to a new mutation rather than one inherited from a person's parents.[2] Angelman syndrome is due to a lack of function of part of chromosome 15 inherited from a person's mother.[2] Most of the time, it is due to a deletion or mutation of the UBE3A gene on that chromosome.[2] Occasionally, it is due to inheriting two copies of chromosome 15 from a person's father and none from their mother.[2] As the father's versions are inactivated by a process known as genomic imprinting, no functional version of the gene remains.[2] Diagnosis is based on symptoms and possibly genetic testing.[3]
No cure is available.[3] Treatment is generally supportive in nature.[3] Anti-seizure medications are used in those with seizures.[3] Physical therapy and bracing may help with walking.[3] Those affected have a nearly normal life expectancy.[2]
AS affects 1 in 12,000 to 20,000 people.[2] Males and females are affected with equal frequency.[3] It is named after a British pediatrician, Harry Angelman, who first described the syndrome in 1965.[3][5] An older term, "happy puppet syndrome", is generally considered pejorative.[6] Prader–Willi syndrome is a separate condition, caused by a similar loss of the father's chromosome 15.[7]
Signs and symptoms
The following text lists signs and symptoms of Angelman syndrome and their relative frequency in affected individuals.[8]
Consistent (100%)
- Developmental delay, functionally severe
- Speech impairment, no or minimal use of words; receptive and non-verbal communication skills higher than verbal ones
- Movement or balance disorder, usually ataxia of gait and/or tremulous movement of limbs
- Behavioral characteristics of the following types: any combination of atypical frequent laughter/smiling; atypically happy demeanor; easily excitable personality, often with hand flapping movements; hypermotoric behavior; short attention span
Frequent (more than 80%)
- Delayed, disproportionate growth in head circumference, usually resulting in microcephaly (absolute or relative) by age 2
- Seizures, onset usually less than 3 years of age
- Abnormal EEG, characteristic pattern with large amplitude slow-spike waves
Associated (20–80%)
- Strabismus
- Hypopigmented skin and eyes
- Tongue thrusting; suck/swallowing disorders
- Hyperactive tendon reflexes
- Feeding problems during infancy
- Uplifted, flexed arms during walking
- Prominent mandible
- Increased sensitivity to heat
- Wide mouth, wide-spaced teeth
- Sleep disturbance
- Frequent drooling, protruding tongue
- Attraction to/fascination with water
- Excessive chewing/mouthing behaviors
- Flat back of head
- Smooth palms
Pathophysiology
Angelman syndrome is caused by the loss of the normal maternal contribution to a region of chromosome 15, most commonly by deletion of a segment of that chromosome. Other causes include uniparental disomy, translocation, or single gene mutation in that region. A healthy person receives two copies of chromosome 15, one from the mother, the other from the father. However, in the region of the chromosome that is critical for Angelman syndrome, the maternal and paternal contribution express certain genes very differently. This is due to sex-specific epigenetic imprinting; the biochemical mechanism is DNA methylation. In a normal individual, the maternal allele of the gene UBE3A,[9] part of the ubiquitin pathway, is expressed and the paternal allele is specifically silenced in the developing brain. In the hippocampus and cerebellum, the maternal allele is almost exclusively the active one. If the maternal contribution is lost or mutated, the result is Angelman syndrome. (Some other genes on chromosome 15 are maternally imprinted, and when the paternal contribution is lost, by similar mechanisms, the result is Prader-Willi syndrome.) The methylation test that is performed for Angelman syndrome (a defect in UBE3A) looks for methylation on the gene's neighbor SNRPN (which is silenced by methylation on the maternal copy of the gene).[10]
While Angelman syndrome can be caused by a single mutation in the UBE3A gene, the most common genetic defect leading to Angelman syndrome is an ~4Mb (mega base) maternal deletion in chromosomal region 15q11-13 causing an absence of UBE3A expression in the paternally imprinted brain regions. UBE3A codes for an E6-AP ubiquitin ligase, which chooses its substrates very selectively, and MAPK1, PMRT5, CDK1, CDK4, β-catenin, and UbxD8 have been identified as ubiquitination targets of this protein.[11]
Initial studies of mice that do not express maternal UBE3A show severe impairments in hippocampal memory formation. Most notably, there is a deficit in a learning paradigm that involves hippocampus-dependent contextual fear conditioning. In addition, maintenance of long-term synaptic plasticity in hippocampal area CA1 in vitro is disrupted in Ube3a−/− mice. These results provide links amongst hippocampal synaptic plasticity in vitro, formation of hippocampus-dependent memory in vivo, and the molecular pathology of Angelman syndrome.
Neurophysiology
The electroencephalogram (EEG) in AS is usually abnormal, more so than clinically expected.[12] This EEG facilitates the differential diagnosis of AS, but is not pathognomonic.[12][13] Three distinct interictal patterns are seen in these patients.[14] The most common pattern is a very large amplitude 2–3 Hz rhythm most prominent in prefrontal leads. Next most common is a symmetrical 4–6 Hz high voltage rhythm. The third pattern, 3–6 Hz activity punctuated by spikes and sharp waves in occipital leads, is associated with eye closure. Paroxysms of laughter have no relation to the EEG, ruling out this feature as a gelastic phenomenon.[12]
EEG anomalies may be used as a quantitative biomarkers to "chart progression of AS and as clinical outcome measures".[15] Slow delta activity (~3 Hz) is greatly increased in AS relative to typically developing children, yet more pronounced in children with partial 15q deletions as opposed to those with etiologies principally affecting UBE3A.[16] Theta activity (~5 Hz) is much greater in children with partial 15q deletions.[16] Thus, delta activity appears to be chiefly reflective of UBE3A dysfunction with some modulation from other 15q genes, whereas theta activity may be an electrophysiological readout of genes beyond UBE3A such as GABRA5, GABRB3, and GABRG3.[16] Future clinical trials in AS might exploit the foregoing by using EEG as a readout of drug target engagement.
It appears that the neurons of people with Angelman syndrome are formed correctly, but they cannot function properly.
Diagnosis
The diagnosis of Angelman syndrome is based on:
- A history of delayed motor milestones and then later a delay in general development, especially of speech
- Unusual movements including fine tremors, jerky limb movements, hand flapping and a wide-based, stiff-legged gait.
- Characteristic facial appearance (but not in all cases).
- A history of epilepsy and an abnormal EEG tracing.
- A happy disposition with frequent laughter
- A deletion or inactivity on chromosome 15 by array comparative genomic hybridization (aCGH) or by BACs-on-Beads technology.
Diagnostic criteria for the disorder were initially established in 1995 in collaboration with the Angelman syndrome Foundation (US);[17] these criteria underwent revision in 2005.[18]
Seizures are a consequence, but so is excessive laughter,[19] which is a major hindrance to early diagnosis.
Differential diagnosis
Treatment
There is currently no cure available. The epilepsy can be controlled by the use of one or more types of anticonvulsant medications. However, there are difficulties in ascertaining the levels and types of anticonvulsant medications needed to establish control, because people with AS often have multiple types of seizures.[20] Many families use melatonin to promote sleep in a condition which often affects sleep patterns. Many individuals with Angelman syndrome sleep for a maximum of five hours at any one time. Mild laxatives are also used frequently to encourage regular bowel movements. Early intervention with physiotherapy is sometimes used to encourage joint mobility and prevent stiffening of the joints. Speech and Language Therapy is commonly employed to assist individuals with Angelman syndrome and their communication issues.
Those with the syndrome are generally happy and contented people who like human contact and play. People with AS exhibit a profound desire for personal interaction with others. Communication can be difficult at first, but as a child with AS develops, there is a definite character and ability to make themselves understood. People with AS tend to develop strong non-verbal skills to compensate for their limited use of speech. It is widely accepted that their understanding of communication directed to them is much larger than their ability to return conversation. Most affected people will not develop more than 5–10 words, if any at all.[21]
Prognosis
The severity of the symptoms associated with Angelman syndrome varies significantly across the population of those affected. Some speech and a greater degree of self-care are possible among the least profoundly affected. Walking and the use of simple sign language may be beyond the reach of the more profoundly affected. Early and continued participation in physical, occupational (related to the development of fine-motor control skills), and communication (speech) therapies are believed to significantly improve the prognosis (in the areas of cognition and communication) of individuals affected by AS. Further, the specific genetic mechanism underlying the condition is thought to correlate to the general prognosis of the affected person. On one end of the spectrum, a mutation to the UBE3A gene is thought to correlate to the least affected, whereas larger deletions on chromosome 15 are thought to correspond to the most affected.
The clinical features of Angelman syndrome alter with age. As adulthood approaches, hyperactivity and poor sleep patterns improve. The seizures decrease in frequency and often cease altogether and the EEG abnormalities are less obvious. Medication is typically advisable to those with seizure disorders. Often overlooked is the contribution of the poor sleep patterns to the frequency and/or severity of the seizures. Medication may be worthwhile to help deal with this issue and improve the prognosis with respect to seizures and sleep. Also noteworthy are the reports that the frequency and severity of seizures temporarily escalate in pubescent Angelman syndrome girls, but do not seem to affect long-term health.The facial features remain recognizable with age, but many adults with AS look remarkably youthful for their age.
Puberty and menstruation begin at around the average age. Sexual development is thought to be unaffected, as evidenced by a single reported case of a woman with Angelman syndrome conceiving a female child who also had Angelman syndrome.[22]
The majority of those with AS achieve continence by day and some by night. Angelman syndrome is not a degenerative syndrome, and thus people with AS may improve their living skills with support.
Dressing skills are variable and usually limited to items of clothing without buttons or zippers. Most adults can eat with a knife or spoon and fork, and can learn to perform simple household tasks. General health is fairly good and life-span near average. Particular problems which have arisen in adults are a tendency to obesity (more in females), and worsening of scoliosis[23] if it is present. The affectionate nature which is also a positive aspect in the younger children may also persist into adult life where it can pose a problem socially, but this problem is not insurmountable.
Epidemiology
Though the prevalence of Angelman syndrome is not precisely known, there are some estimates. The best data available are from studies of school age children, ages 6–13 years, living in Sweden and from Denmark where the diagnosis of AS children in medical clinics was compared to an 8-year period of about 45,000 births. The Swedish study showed an AS prevalence of about 1/20,000[24] and the Danish study showed a minimum AS prevalence of about 1/10,000.[25]
History
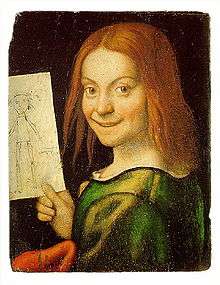
Harry Angelman, a pediatrician working in Warrington, England, first reported three children with this condition in 1965.[5] Angelman later described his choice of the title "Puppet Children" to describe these cases as being related to an oil painting he had seen while vacationing in Italy:
The history of medicine is full of interesting stories about the discovery of illnesses. The saga of Angelman's syndrome is one such story. It was purely by chance that nearly thirty years ago (e.g., circa 1964) three handicapped children were admitted at various times to my children's ward in England. They had a variety of disabilities and although at first sight they seemed to be suffering from different conditions I felt that there was a common cause for their illness. The diagnosis was purely a clinical one because in spite of technical investigations which today are more refined I was unable to establish scientific proof that the three children all had the same handicap. In view of this I hesitated to write about them in the medical journals. However, when on holiday in Italy I happened to see an oil painting in the Castelvecchio Museum in Verona called ... a Boy with a Puppet. The boy's laughing face and the fact that my patients exhibited jerky movements gave me the idea of writing an article about the three children with a title of Puppet Children. It was not a name that pleased all parents but it served as a means of combining the three little patients into a single group. Later the name was changed to Angelman syndrome. This article was published in 1965 and after some initial interest lay almost forgotten until the early eighties.
— Angelman quoted by Charles Williams[27]
Case reports from the United States first began appearing in the medical literature in the early 1980s.[28][29] In 1987, it was first noted that around half of the children with AS have a small piece of chromosome 15 missing (chromosome 15q partial deletion).[30]
Society and culture
Many poems in Richard Price's poetry collections Hand Held (1997), Lucky Day (2005), and Small World (2012) reflect on the disability of the poet's daughter, who has Angelman syndrome. In the 2011 Philippine drama series Budoy, the titular character and main protagonist Budoy Maniego (played by Filipino actor Gerald Anderson) is diagnosed with Angelman syndrome.
Research
Topoisomerase inhibitors are under research as of 2017.[31]
References
- Winter, Robin M.; Baraitser, Michael (2013). Multiple Congenital Anomalies: A Diagnostic Compendium. Springer. p. 34. ISBN 9781489931092. Archived from the original on 2017-11-05.
- Reference, Genetics Home (May 2015). "Angelman syndrome". Genetics Home Reference. Archived from the original on 27 August 2016. Retrieved 28 April 2017.
- "Angelman Syndrome – NORD (National Organization for Rare Disorders)". NORD (National Organization for Rare Disorders). 2015. Archived from the original on 13 November 2016. Retrieved 28 April 2017.
- "Common Misdiagnoses | FAST". FAST (Foundation for Angelman Syndrome Therapeutics). Retrieved 10 October 2019.
- Angelman, Harry (1965). "'Puppet' Children: A report of three cases". Dev Med Child Neurol. 7 (6): 681–688. doi:10.1111/j.1469-8749.1965.tb07844.x.
- Wilson, Golder N.; Cooley, W. Carl (2000). Preventive Management of Children with Congenital Anomalies and Syndromes. Cambridge University Press. p. 193. ISBN 9780521776738. Archived from the original on 2017-11-05.
- Kumar, Vinay; Abbas, Abul K.; Aster, Jon C. (2013). Robbins Basic Pathology. Elsevier Health Sciences. p. 244. ISBN 978-1437717815. Archived from the original on 2017-11-05.
- Facts about Angelman syndrome (PDF) Archived May 27, 2013, at the Wayback Machine. Anonymous. Angelman syndrome Foundation (US) website. Retrieved September 29, 2012.
- Weeber E, Levenson J, Sweatt J (2002). "Molecular genetics of human cognition". Mol Interv. 2 (6): 376–91, 339. doi:10.1124/mi.2.6.376. PMID 14993414.
- White HE, Durston VJ, Harvey JF, Cross NC (2006). "Quantitative analysis of SNRPN(correction of SRNPN) gene methylation by pyrosequencing as a diagnostic test for Prader-Willi syndrome and Angelman syndrome". Clin. Chem. 52 (6): 1005–13. doi:10.1373/clinchem.2005.065086. PMID 16574761.
- Wang, Yiyang, et al. (2017). "Identifying the ubiquitination targets of E6AP by orthogonal ubiquitin transfer". Nature Communications. 8 (1): 2232. Bibcode:2017NatCo...8.2232W. doi:10.1038/s41467-017-01974-7. PMC 5738348. PMID 29263404.
- Williams C (2005) "Neurological aspects of the Angelman syndrome" Brain & Development 27: 88–94
- Laan, Laura A.E.M.; Vein, Alla A. (2005). "Angelman syndrome: is there a characteristic EEG?". Brain and Development. 27 (2): 80–87. doi:10.1016/j.braindev.2003.09.013. ISSN 0387-7604. PMID 15668045.
- Dan, B., Angelman syndrome: Current understanding and research prospects. Epilepsia, 2009. 50(11): p. 2331–2339.
- Sidorov, Michael S.; Deck, Gina M.; Dolatshahi, Marjan; Thibert, Ronald L.; Bird, Lynne M.; Chu, Catherine J.; Philpot, Benjamin D. (2017-05-08). "Delta rhythmicity is a reliable EEG biomarker in Angelman syndrome: a parallel mouse and human analysis". Journal of Neurodevelopmental Disorders. 9: 17. doi:10.1186/s11689-017-9195-8. ISSN 1866-1955. PMC 5422949. PMID 28503211.
- Frohlich, Joel, Meghan Miller, Lynne M. Bird, Pilar Garces, Hannah Purtell, Marius C. Hoener, Benjamin D. Philpot et al. "Electrophysiological phenotype in Angelman syndrome differs between genotypes." Biological Psychiatry (2019).
- Williams CA, Angelman H, Clayton-Smith J, et al. (1995). "Angelman syndrome: consensus for diagnostic criteria. Angelman syndrome Foundation". Am. J. Med. Genet. 56 (2): 237–8. doi:10.1002/ajmg.1320560224. PMID 7625452.
- Williams CA, Beaudet AL, Clayton-Smith J, et al. (2006). "Angelman syndrome 2005: updated consensus for diagnostic criteria". Am. J. Med. Genet. A. 140 (5): 413–8. doi:10.1002/ajmg.a.31074. PMID 16470747.
- Buntinx IM, Hennekam RC, Brouwer OF, et al. (March 1995). "Clinical profile of Angelman syndrome at different ages". American Journal of Medical Genetics. 56 (2): 176–83. doi:10.1002/ajmg.1320560213. PMID 7625442.
- Leung, HT; Ring, H (January 2013). "Epilepsy in four genetically determined syndromes of intellectual disability". Journal of Intellectual Disability Research : JIDR. 57 (1): 3–20. doi:10.1111/j.1365-2788.2011.01505.x. PMID 22142420.
- Andersen WH, Rasmussen RK, Strømme P (2001). "Levels of cognitive and linguistic development in Angelman syndrome: a study of 20 children". Logopedics, Phoniatrics, Vocology. 26 (1): 2–9. doi:10.1080/140154301300109044. PMID 11432411.
- Lossie A, Driscoll D (1999). "Transmission of Angelman syndrome by an affected mother". Genet Med. 1 (6): 262–6. doi:10.1097/00125817-199909000-00004. PMID 11258627.
- Laan LA, den Boer AT, Hennekam RC, Renier WO, Brouwer OF (1996). "Angelman syndrome in adulthood". Am. J. Med. Genet. 66 (3): 356–60. doi:10.1002/(SICI)1096-8628(19961218)66:3<356::AID-AJMG21>3.0.CO;2-K. hdl:2066/22929. PMID 9072912.
- Steffenburg S, Gillberg CL, Steffenburg U, Kyllerman M (1996). "Autism in Angelman syndrome: a population-based study". Pediatr. Neurol. 14 (2): 131–6. doi:10.1016/0887-8994(96)00011-2. PMID 8703225.
- Petersen MB, Brøndum-Nielsen K, Hansen LK, Wulff K (1995). "Clinical, cytogenetic, and molecular diagnosis of Angelman syndrome: estimated prevalence rate in a Danish county; the disorder predominantly affects Anglo-Saxons". Am. J. Med. Genet. 60 (3): 261–2. doi:10.1002/ajmg.1320600317. PMID 7573182.
- Galassi FM, Armocida E, Rühli FJ (September 2016). "Angelman Syndrome in the Portrait of a Child With a Drawing by Giovanni F. Caroto" (PDF). JAMA Pediatr. 170 (9): 831. doi:10.1001/jamapediatrics.2016.0581. PMID 27380555.CS1 maint: uses authors parameter (link)
- Williams, Charles. "Harry Angelman and the History of AS". Stay informed. US: Angelman Syndrome Foundation. Archived from the original on 2011-06-30. Retrieved 2011-07-01.
- Dooley, JM; Berg JM; Pakula Z; MacGregor DL. (1981). "The puppet-like syndrome of Angelman". Am J Dis Child. 135 (7): 621–4. doi:10.1001/archpedi.1981.02130310027010. PMID 7246489.
- Williams, CA; Frias JL (1982). "The Angelman ("happy puppet") syndrome". Am J Med Genet. 11 (4): 453–60. doi:10.1002/ajmg.1320110411. PMID 7091188.
- Magenis, RE; Brown MG; Lacy DA; Budden S; LaFranchi S. (1987). "Is Angelman syndrome an alternate result of del(15)(q11q13)?". Am J Med Genet. 28 (4): 829–38. doi:10.1002/ajmg.1320280407. PMID 3688021.
- Tan, WH; Bird, LM (June 2017). "Pharmacological therapies for Angelman syndrome". Wiener medizinische Wochenschrift. 167 (9–10): 205–218. doi:10.1007/s10354-015-0408-z. PMID 26758979.
External links
| Classification | |
|---|---|
| External resources |
|
| Wikimedia Commons has media related to Angelman syndrome. |