Adie syndrome
Adie syndrome also known as the Holmes-Adie syndrome is a neurological disorder characterized by a tonically dilated pupil that reacts slowly to light but shows a more definite response to accommodation (i.e., light-near dissociation).[1] It is frequently seen in females with absent knee or ankle jerks and impaired sweating. It is named after the British neurologists William John Adie and Gordon Morgan Holmes who independently described the same disease in 1931.[2] It is caused by damage to the postganglionic fibers of the parasympathetic innervation of the eye, usually by a viral or bacterial infection which causes inflammation, and affects the pupil of the eye and the autonomic nervous system.[1]
| Adie's syndrome | |
|---|---|
| Other names | Holmes–Adie syndrome, Adie's tonic pupil, Holmes-Adie pupil |
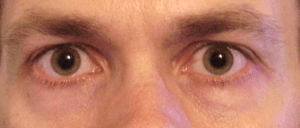 | |
| Bilateral mydriasis given the observational diagnosis Adie's pupils by an ophthalmologist | |
| Pronunciation |
|
| Specialty | Ophthalmology |
Signs and symptoms
Adie syndrome presents with three hallmark symptoms, namely at least one abnormally dilated pupil (mydriasis) which does not constrict in response to light, loss of deep tendon reflexes, and abnormalities of sweating.[1] Other signs may include hyperopia due to accommodative paresis, photophobia and difficulty reading.[3] Some individual with Adie syndrome may also have cardiovascular abnormalities.[4]
Pathophysiology
Pupillary symptoms of Holmes–Adie syndrome are thought to be the result of a viral or bacterial infection that causes inflammation and damage to neurons in the ciliary ganglion, located in the posterior orbit, that provides parasympathetic control of eye constriction. Additionally, patients with Holmes-Adie Syndrome can also experience problems with autonomic control of the body. This second set of symptoms is caused by damage to the dorsal root ganglia of the spinal cord. Adie's pupil is supersensitive to ACh so agonist like pilocarpine whose dose would not be able to cause pupil constriction in normal patient would cause it in this patient. The circuitry for the pupillary constriction does not descend below upper midbrain, henceforth impaired pupillary constriction is extremely important to detect as it can be early sign of the brainstem herniation[1]
Diagnosis
Clinical exam may reveal sectoral paresis of the iris sphincter or vermiform iris movements. The tonic pupil may become smaller (miotic) over time which is referred to as "little old Adie's".[5] Testing with low dose (1/8%) pilocarpine may constrict the tonic pupil due to cholinergic denervation supersensitivity.[1] A normal pupil will not constrict with the dilute dose of pilocarpine.[5] CT scans and MRI scans may be useful in the diagnostic testing of focal hypoactive reflexes.[6]
Treatment
The usual treatment of a standardised Adie syndrome is to prescribe reading glasses to correct for impairment of the eye(s).[1] Pilocarpine drops may be administered as a treatment as well as a diagnostic measure.[1] Thoracic sympathectomy is the definitive treatment of diaphoresis, if the condition is not treatable by drug therapy.[1]
Prognosis
Adie's syndrome is not life-threatening or disabling.[1] As such, there is no mortality rate relating to the condition; however, loss of deep tendon reflexes is permanent and may progress over time.[1]
Epidemiology
It most commonly affects younger women (2.6:1 female preponderance) and is unilateral in 80% of cases.[5] Average age of onset is 32 years.
See also
References
- "Holmes-Adie syndrome Information Page". National Institute of Neurological Disorders and Stroke. Archived from the original on 2007-10-16. Retrieved 2008-01-21.
- Siddiqui AA, Clarke JC, Grzybowski A (November 2014). "William John Adie: the man behind the syndrome" (PDF). Clinical & Experimental Ophthalmology. 42 (8): 778–84. doi:10.1111/ceo.12301. PMID 24533698.
- Stedman's Medical Dictionary (27th ed.). 2000. ISBN 978-0-683-40007-6.
- "Adie syndrome". Genetic and Rare Diseases Information Center (GARD) – an NCATS Program.
- Haines DE (2002). Fundamental Neuroscience, 2nd edition. ISBN 978-0-443-06603-0.
- "Diagnosis of Adie syndrome WrongDiagnosis.com". Retrieved 2008-01-21.
Further reading
- Estañol B, Callejas-Rojas RC, Cortés S, Martínez-Memije R, Infante-Vázquez O, Delgado-García G (2017). "Asymptomatic Severe Vagal and Sympathetic Cardiac Denervation in Holmes-Adie's Syndrome". Case Reports in Neurological Medicine. 2017: 4919758. doi:10.1155/2017/4919758. PMC 5385912. PMID 28428900.