46,XX testicular disorders of sex development
46,XX testicular disorders of sex development (46,XX DSD) describes a condition in which individuals with two X chromosomes in each cell, the pattern typically found in females, have a male phenotype appearance.[1][2] 46,XX testicular disorders of sex development may also be named 46,XX sex reversal, nonsyndromic 46,XX testicular DSD, XX male syndrome, and XX sex reversal.[3]
| 46,XX testicular disorders of sex development | |
|---|---|
| Other names | De la Chapelle syndrome |
_Karyotype_Human_46%2CXX_(woman).jpg) | |
| Human karyotype 46 XX | |
Presentation
People with 46,XX testicular DSD have male external genitalia. They generally have small testes and may also have abnormalities such as undescended testes (cryptorchidism) or the urethra opening on the underside of the penis (hypospadias). A small number of affected people have external genitalia that do not look clearly male or clearly female (ambiguous genitalia). Affected children are typically raised as males and are likely to have a male gender identity.[3]
Cause
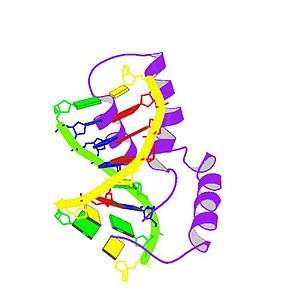
In about 80 percent of individuals with 46,XX testicular disorder of sex development, the condition results from an abnormal exchange of genetic material between chromosomes (translocation). This exchange occurs as a random event during the formation of sperm cells in the affected person's father. The translocation causes the SRY gene to be misplaced, almost always onto an X chromosome. If a fetus is conceived from a sperm cell with an X chromosome bearing the SRY gene, it will develop as a male despite not having a Y chromosome. This form of the condition is called SRY-positive 46,XX testicular disorder of sex development.[3]
About 20 percent of those with 46 XX testicular disorder of sex development do not have the SRY gene. This form of the condition is called SRY-negative 46,XX testicular disorder of sex development. The cause of the disorder in these individuals is often unknown, although changes affecting other genes have been identified. Individuals with SRY-negative 46,XX testicular disorder of sex development are more likely to have ambiguous genitalia than are people with the SRY-positive form.[3]
Diagnosis
Cytogenetic testing shows the presence of the 46,XX karyotype.[4]
Treatment
At puberty, most affected individuals require treatment with the male sex hormone testosterone to induce development of male secondary sex characteristics such as facial hair and deepening of the voice (masculinization). Hormone treatment can also help prevent breast enlargement (gynecomastia). Adults with this disorder are usually shorter than average for males and are unable to have children (infertile).[3]
Epidemiology
Approximately 1 in 20,000 individuals with a male appearance have 46,XX testicular disorder.[3]
References
- RESERVED, INSERM US14 -- ALL RIGHTS. "Orphanet: 46,XX testicular disorder of sex development". www.orpha.net. Retrieved 2017-01-12.
- Délot, EC; Vilain, EJ; Pagon, RA; Adam, MP; Ardinger, HH; Wallace, SE; Amemiya, A; Bean, LJH; Bird, TD; Fong, CT; Mefford, HC; Smith, RJH; Stephens, K (1993). "Nonsyndromic 46,XX Testicular Disorders of Sex Development". GeneReviews. University of Washington, Seattle. PMID 20301589. Retrieved 12 January 2017.updated 2015
- "46,XX testicular disorder of sex development - Genetics Home Reference". Retrieved 2017-01-08.

- Délot, Emmanuèle C; Vilain, Eric J (2003). "Nonsyndromic 46,XX Testicular Disorders of Sex Development". GeneReviews. Retrieved 6 December 2018.
Further reading
- "Ambiguous Genitalia. Uncertain genetalia information. Patient | Patient". Patient. Retrieved 12 January 2017.
External links
| Classification |
|
|---|---|
| External resources |
|